



Introduction
Compulsivity is the tendency to engage in repetitive, habitual, or ritualistic behaviors.Reference Albertella, Chamberlain and Le Pelley 1 Such behaviors are carried out by individuals to abide by existing cognitive rules and the sense that these behaviors must be completed, despite the individual’s awareness that these behaviors do not align with their overall goals.Reference Luigjes, Lorenzetti and De Haan 2 High compulsivity is correlated with a number of psychiatric disorders. Conditions characterized by high compulsivity include - but are not limited to - clinical and subclinical symptoms of obsessive–compulsive disorder (OCD), body dysmorphic disorder, hoarding disorder (HD), trichotillomania (hair pulling disorder), excoriation (skin-picking) disorder, and disorders due to addictive behaviors such as substance use and gambling disorders.Reference Fontenelle, Oldenhof and Eduarda Moreira-De-Oliveira 3 , Reference Yücel, Oldenhof and Ahmed 4 As well as compulsivity, increased psychological distress has been shown to be a key driver of transdiagnostic compulsive behaviors in community samples.Reference Albertella, Rotaru and Christensen 5 , Reference Den Ouden, Tiego and RSC 6
The poor physical health of people living with mental illness has been reported globally, regardless of socioeconomic status.Reference Firth, Siddiqi and Koyanagi 7 While this field of research has assessed an array of factors, those lifestyle factors commonly linked with mental health include diet quality, sleep quality, and physical activity.Reference Firth, Ward and Stubbs 8 Disorders involving compulsive behaviors are no exception, and the high prevalence of unhealthy lifestyle behaviors of individuals with compulsive disorders has been well documented.Reference Fontenelle, Zeni-Graiff, Quintas and Yucel 9
For instance, a review of sleep in obsessive–compulsive and related disorders (OCRDs) detected a general trend of increased sleep disturbance in people experiencing OCRDs, with sleep disturbance being more common in OCD and HD.Reference Cox, Parmar and Olatunji 10 Further, higher sugar and fat intake is shown to be significantly associated with greater gambling pathology,Reference Chamberlain, Redden and Grant 11 while robust randomized controlled trials have shown the nutrient supplement n-acetylcysteine (commonly found in protein-rich foods) to improve symptoms across OCRDs spectrum alongside standard treatment.Reference Brierley, Thompson, Albertella and Fontenelle 12 - Reference Grant, Chamberlain, Redden, Leppink, Odlaug and Kim 15 While many studies have relied on cross-sectional data and we therefore cannot infer causal association between lifestyle and compulsive behaviors, causal links between diet factors and OCD-like behaviors have been shown in animal models.Reference Kantak, Bobrow and Nyby 16 , Reference Magnusson, Hauck and Jeffrey 17 Research has suggested that individuals with OCD (and without depression) present with a less varied gut microbiome and higher inflammation levels when compared to a nonpsychiatric control group.Reference Turna, Grosman Kaplan and Anglin 18 , Reference Domènech, Willis and Alemany 19 This evidence supports theoretical models linking the microbiome—influenced by a range of lifestyle factors—and compulsivity.Reference Magnusson, Hauck and Jeffrey 17 , Reference Turna, Kaplan, Anglin and Ameringen 20
The evidence surrounding physical activity and compulsivity remains mixed. For instance, cross-sectional studies have not revealed a relationship between exercise and OCDReference Freedman and Richter 21 and, in fact, alcohol use disorder (excluding severe forms) has been associated with higher levels of physical activity.Reference Lisha, Sussman, Fapa and Leventhal 22 Yet, acute decreases in OCD symptoms have been reported by participants of moderate intensity physical exercise interventionsReference Abrantes, Strong and Cohn 23 , Reference Abrantes, Farris and Brown 24 (for a review see Reference Reference Brierley, Thompson, Albertella and Fontenelle12). More generally, physical activity is positively associated with broad mental health outcomes including anxiety and depression.Reference Schuch, Vancampfort and Firth 25 , Reference Stubbs, Koyanagi and Hallgren 26 Further research is needed in a general population to tease apart the relationships between mental health or psychological distress, physical activity, and compulsivity.
Emerging evidence indicates lifestyle factors play a key role in general mental wellbeing through common mechanisms of action which influence psychological distress in community and clinical samples. Low levels of brain-derived neurotrophic factor (BDNF; an important protein for neuroplasticity and mental wellbeing) have been reported amongst individuals engaging in compulsive behaviors.Reference Maina, Rosso, Zanardini, Bogetto, Gennarelli and Bocchio-Chiavetto 27 , Reference Wang, Mathews, Li, Lin and Xiao 28 To counter this, BDNF levels can be increased—and, potentially, compulsivity may be decreased—through engagement in high-intensity physical activity,Reference Dinoff, Herrmann, Swardfager and Lanctôt 29 diet quality,Reference Haghighat, Rajabi and Mohammadshahi 30 , Reference Molteni, Barnard, Ying, Roberts and Gómez-Pinilla 31 and sleep quality improvements through a reduction in psychological distress.Reference Schmitt, Holsboer-Trachsler and Eckert 32 , Reference Giese, Unternaehrer, Brand, Calabrese, Holsboer-Trachsler and Eckert 33 Analyzing these lifestyle factors, especially in combination, will be valuable in understanding whether they impact similar mental health constructs such as psychological distress and compulsivity. As lifestyle and mental health factors can differ across cultures, studying these relationships in multiple independent samples is important in understanding whether there may be a consistency across the mechanisms influencing the relationship between lifestyle and compulsivity.
Psychological distress has been reliably linked to a number of lifestyle factors including diet quality and dietary patterns, including adherence to a Mediterranean diet,Reference Francis, Stevenson, Chambers, Gupta, Newey and Lim 34 - Reference Sadeghi, Keshteli, Afshar, Esmaillzadeh and Adibi 36 amount of physical activityReference Perales, Pozo-Cruz and Pozo-Cruz 37 , Reference Sloan, Sawada, Girdano, Liu, SJH and Blair 38 and sleep quality.Reference João, SND, Carmo and Pinto 39 Yet, the direction of the relationship between compulsivity and lifestyle requires further investigation. It is unknown, for instance, whether unhealthy/poor quality lifestyle behaviors increase compulsivity directly (through an effect on cognitive mechanisms underlying behavior), whether compulsivity leads to unhealthy/poor quality lifestyle behaviors by interfering directly with healthier daily activities (eg, less sleep time due to compulsions being carried out late into the evening),Reference Fontenelle, Zeni-Graiff, Quintas and Yucel 9 or whether this relationship may be mediated by other factors, including psychological distress. This holds important implications for therapeutic targets for preventing and treating compulsive disorders, as well as informing the true transdiagnostic nature and potential of lifestyle-based interventions.
This study has two aims: (a) To assess the relationship between lifestyle factors (specifically diet quality, sleep quality and level of physical activity) and transdiagnostic compulsivity; and (b) To assess whether the relationship between lifestyle factors and compulsivity is statistically accounted for by psychological distress. Considering that lifestyles, compulsivity levels and distress related to these factors may be different across cultures, we attempted to determine the reliability and generalizability of our results in a cross-sectional design using two independent community samples.
Methods
We conducted two independent, online, cross-sectional questionnaire studies in accordance with the Declaration of Helsinki. The Monash University Human Research Ethics Committee reviewed and approved both studies.
Participants
Across both samples, eligible participants were adults (18 years and over).
Sample one: United States
As reported previously,Reference Fontenelle, Albertella and Brierley 40 , Reference Fontenelle, Destrée and Brierley 41 we recruited 829 participants residing in the United States of America in July 2020 through Amazon Mechanical Turk, an online crowdsourcing platform targeting US participants. Participants were reimbursed US$15. We restricted our recruitment to participants whose first language was English or who reported learning English before the age of seven, and used the Approved Participants function on CloudResearch to only include participants who have passed previous attention and engagement measures distributed by the platform.
Sample two: Australia
As reported previously,Reference Albertella, Rotaru and Christensen 5 we recruited 992 participants throughout Australia from May–July 2020 primarily through Prolific (n = 698)—an online crowdsourcing platform—and used the custom prescreening function to recruit only participants residing in Australia. The remaining participants (n = 294) were recruited through social media advertisements. Participants recruited through Prolific received reimbursement of £7.50 per hour. We offered participants completing the questionnaire through other means entry into a draw to win one of 50 AU$100 vouchers for a department store.
Measures
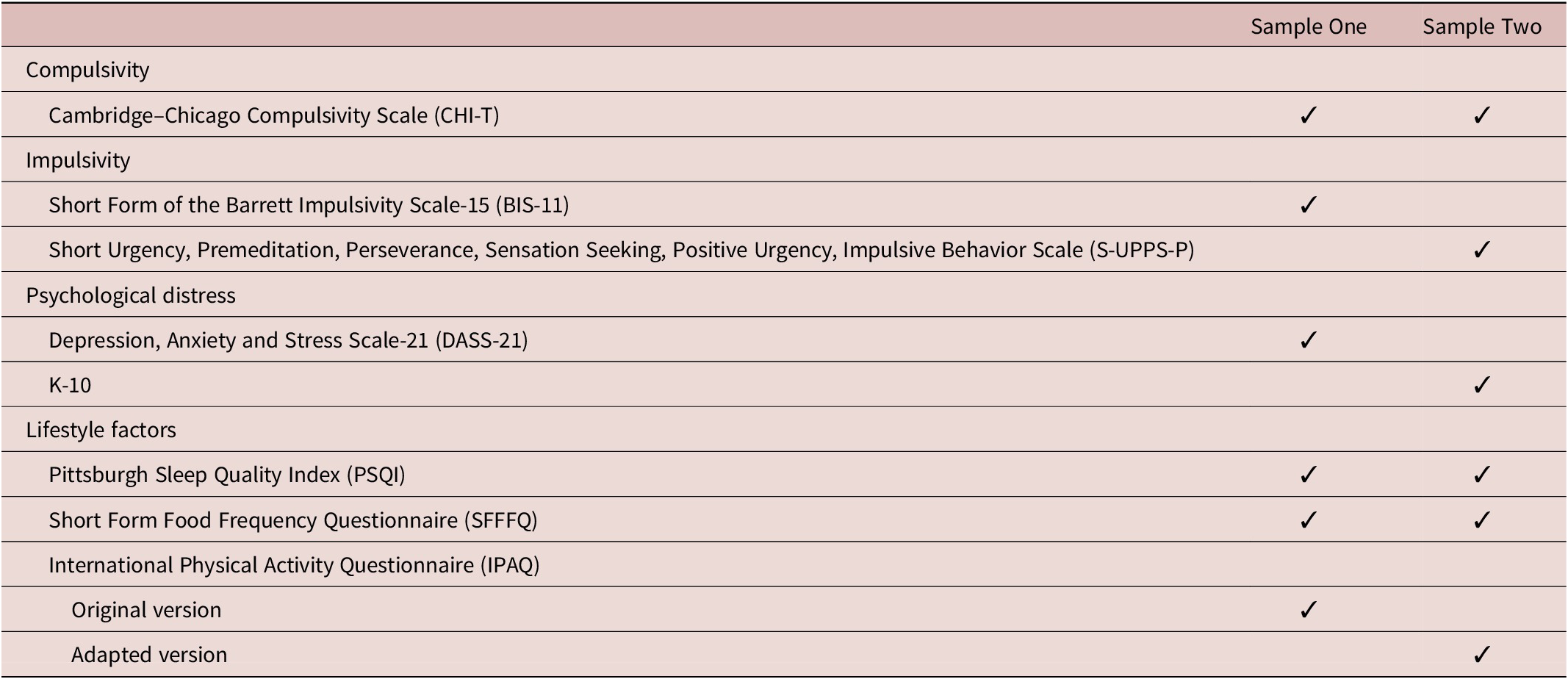
Participants in both samples provided demographic information including their age, sex, and employment status, and completed a series of questionnaires related to psychiatric history, personality factors, lifestyle, and obsessive–compulsive symptoms (Table 1 and outlined in text below). Unless stated otherwise, the below measures were applied across both samples.
Table 1. Constructs and Corresponding Instruments Completed by Each Sample
Compulsivity
Cambridge–Chicago Compulsivity Scale (CHI-T)
The CHI-T measures compulsivity across 15 statements.Reference Chamberlain and Grant 42 Item response options range from strongly disagree (0) to strongly agree (3). The CHI-T total score—the score of interest for this study—ranges from 0 to 45 with higher scores indicating higher compulsivity. The CHI-T shows concurrent validity with the Padua Inventory (a scale for the measurement of Obsessive–Compulsive symptoms) and the Structured Clinical Interview for Gambling Disorder.Reference Chamberlain and Grant 42 The CHI-T is often used as a measure of symptom severity across transdiagnostic compulsive disorders.Reference Hook, Grant and Ioannidis 43
Impulsivity
Short form of the Barrett Impulsivity Scale-15 (BIS-15)
The BIS-15 is a 15-item scale measuring impulsivity. It has been widely used in community samples and shown a 3-factor structure of nonplanning, motor impulsivity, and attention impulsivity. Psychometric properties support the BIS-15 as a valid and reliable measure of impulsivity.Reference Spinella 44 We used the BIS-15 total score (15–60), and this measure was completed by Sample One only.
Short Urgency, Premeditation, Perseverance, Sensation Seeking, Positive Urgency, Impulsive Behavior Scale (S-UPPS-P)
The S-UPPS-P is a 20 item measure with five subscales relating to different domains of impulsivity.Reference Cyders, Littlefield, Coffey and Karyadi 45 Participants are required to rate their level of agreement with statements regarding how they generally think and act. Total scores range from 20 to 80 where higher scores indicate greater levels of impulsivity. We referred to the UPPS-P total score, and this was completed by Sample Two only.
Psychological distress
Depression, Anxiety and Stress Scale-21 (DASS-21)
The DASS-21 is an established measure of psychological functioningReference Antony, Bieling, Cox, Enns and Swinson 46 through negative emotional states of depression, anxiety, and stress.Reference Lovibond and Lovibond 47 Participants select a response from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time) response indicating how they have felt in the past week. The DASS-21 total score was the measure of interest for our study, and this measure was used for Sample One only.
K10
The K10 is a 10-item measure of psychological distress over the past month.Reference Kessler, Andrews and Colpe 48 Participants are asked to rate their level of distress (eg, “About how often did you feel hopeless”) on a five-point Likert scale. The K10 total score was the measure of interest for our study, and this measure was used for Sample Two only.
Lifestyle factors
Pittsburgh Sleep Quality Index (PSQI)
The PSQI measures sleep quality considering several domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of medication, and daytime dysfunction.Reference Buysse, Reynolds, Monk, Berman and Kupfer 49 Scoring is based on a four-point Likert scale and total scores range from 0 to 42 with higher scores indicating poorer sleep quality. The PSQI demonstrates high internal consistency (α = 0.83). We referred to the total score in the current study.
Short Form Food Frequency Questionnaire (SFFFQ)
The SFFFQ measures diet quality based on the respondent’s reported food and drink intake over a typical week in the past month.Reference Cleghorn, Harrison, Ransley, Wilkinson, Thomas and Cade 50 Responses are given on a 6- to 8-point Likert scale ranging from “rarely or never” to “5+ a day” or “7+ a week.” The SFFFQ was developed for use in a British population, however, we adapted the measure and employed language more appropriate to use in the United States of America and Australia for the respective samples. Data from the SFFFQ is represented by an overall Diet Quality Score (DQS)—the score of interest for this study—with a highest possible score of 15.
International Physical Activity Questionnaire (IPAQ)
The IPAQ is a short measure of physical activity based on participant recall from the 7 days prior.Reference Craig, Marshall and Sjöström 51 Participants are asked to provide the number of days they engaged in vigorous intensity physical activity, moderate intensity physical activity and walking, with example of each of these provided (eg, “During the last 7 days, on how many days did you do vigorous physical activities like heavy lifting, digging, aerobics, or fast bicycling?”). Participants are also asked to record how long they usually spent doing each of these activities, with reference to one of the days (eg, “How much time did you usually spend doing vigorous physical activities on one of those days?”). Participants are also asked to provide their average sitting time each day. Vigorous, moderate and walking physical activity is converted to metabolic equivalent of task (MET) minutes and totalled to provide a single MET minutes scores for each participant. This version of the IPAQ was for Sample One.
For Sample Two, we used an adapted version of the IPAQ wherein participants who recorded any days of vigorous, moderate, or low intensity activity were asked to state the estimated number of minutes they were engaged in the respective activities for each of these days. We then converted recorded physical activity time to MET minutes.
Data analysis
We performed statistical analyses using SPSS Version 26 and the PROCESS macro (see below for further statistical details).Reference Preacher and Hayes 52 We obtained descriptive statistics for each sample (age, sex, and employment status), and undertook analyses for the two studies independently from one another.
At the data analysis stage, we removed participants who did not complete all study measures relevant to our analyses. Following removal of cases with missing data, we independently analyzed data from 749 participants in Sample One and 796 participants in Sample Two. We ran independent samples t tests, or chi-square tests where appropriate, to test for statistically significant differences between the two groups in terms of age, gender, employment, compulsivity, and lifestyle factors. Due to differing instruments used to measure impulsivity and psychological distress, it was not possible to test for a statistically significant difference between groups on these constructs.
We performed six mediation analyses on each sample. Initially, sleep quality, diet quality, and physical activity formed predictor variables. Psychological distress was defined as a candidate mediating variable and compulsivity was the outcome variable. As we used cross-sectional data in which causality cannot be assumed, we also ran mediation analyses with sleep quality, diet quality, and physical activity forming outcome variables, compulsivity being the predictor variable and psychological distress remaining the mediator.
We controlled for impulsivity, age and sex across all analyses by adding these variables into the mediation models as covariates. Of note, we controlled for impulsivity as a possible confound on the relationships between lifestyle, psychological distress, and compulsivity. Past research has shown impulsivity to be highly correlated with compulsivity and to influence psychological distress.Reference Albertella, Chamberlain and Le Pelley 1 , Reference Fontenelle, Destrée and Brierley 41 , Reference Chamberlain, Stochl, Redden and Grant 53 , Reference Shin, Hong and Jeon 54 We adopted an error rate of P < .05 to determine significance of total and direct effects in the mediation analyses, and the bootstrapping method to determine significance of the indirect effect, and therefore the existence of mediation in the model. Using the bootstrapping method, the indirect effect is deemed significant when the confidence interval of the bootstrapped distribution does not pass through zero.Reference Hayes and Rockwood 55 We referred to the unstandardized coefficient beta (b) to determine effect sizes. In this study, we used the CHI-T, typically a measure of compulsivity, as an indicator of transdiagnostic symptom severity. To confirm that data from both samples are consistent with previous research stating that higher compulsivity is associated with greater compulsive psychopathology,Reference Chamberlain and Grant 42 we ran the same mediation analyses as stated above, replacing the CHI-T with a measure of obsessive–compulsive symptom severity (ie, the DOCS from Sample One and the OCI-R from Sample Two). Please see Supplementary Material for these results.
Results
Please refer to Table 2 for participant characteristics. Compared to participants in Sample One, those in Sample Two were significantly younger in age, less likely to be employed full-time, more likely to endorse another form of employment (eg, casual or part-time employment, or study) or to be unemployed. Additionally, more participants in Sample Two identified as a gender other than male or female than those in Sample One. Participants in Sample Two reported significantly higher levels of compulsivity, higher diet quality and less physical activity than those in Sample One.
Table 2. Participant Characteristics

* Indicates significant differences between groups at P < .01.
** Indicates significant differences between groups at P < .05.
We present results of mediation analyses below with lifestyle factors as predictors of compulsivity in Table 3, and compulsivity as a predictor of lifestyle factors in Table 4. Please also see Supplementary Material for mediation analyses examining the relationship between obsessive–compulsive symptom severity (DOCS and OCI-R) and lifestyle factors. Generally, examination of the relationship between obsessive–compulsive symptom severity and lifestyle factors mirrored findings from our compulsivity analyses.
Table 3. Mediation Results of the Effect of Lifestyle Factors on Compulsivity, Mediated by Psychological Distress

Note: Predictor variable: lifestyle factors as stated in the table; Outcome variables: compulsivity; Mediator variable: psychological distress; MET: metabolic equivalents of task. Significant values are bolded.
Table 4. Mediation Results of the Effect of Compulsivity on Lifestyle Factors, Mediated by Psychological Distress

Note: Predictor variable: compulsivity; Outcome variables: lifestyle factors as stated in the table; Mediator variable: psychological distress; MET: metabolic equivalents of task. Significant values are bolded.
Sleep and compulsivity
Figure 1 shows sleep quality as a predictor of compulsivity is mediated through psychological distress. Through mediation analyses on Sample One, we found the total effect of sleep quality on compulsivity to be significant (c path; b = 0.2910, t(744) = 5.8564, P < .0001). The direct effect of sleep quality on compulsivity was not significant after accounting for distress (c΄ path; b = 0.0797, t(744) = 1.2929, P = .1965) while the indirect effect of sleep on compulsivity was significant (a and b paths multiplied; b = 0.2113, 95% Confidence Interval [CI] = 0.1312–0.2961).

Figure 1. Sleep quality and compulsivity mediation models for Studies One (left) and Two (right). **Significant results at P < .01 level. Solid lines indicate model where sleep quality predicts compulsivity, mediated by distress. Dashed lines indicate model where compulsivity predicts sleep quality, mediated by distress.
In Sample Two, we found the total effect of sleep quality on compulsivity to be significant (c path; b = 0.2673, t(791) = 5.0817, P < .0001). The direct effect of sleep quality on compulsivity was not significant after accounting for distress (c΄ path; b = −0.0041, t(791) = −0.0696, P = .9445), and the indirect effect of sleep on compulsivity was significant (a and b paths multiplied; b = 0.2713, 95% CI = 0.2031–0.3439). Taken together, our findings from Studies One and Two were consistent and indicate that psychological distress is an important explanatory variable linking sleep quality and compulsivity.
When entering compulsivity as the predictor variable, we found these results to be bidirectional whereby psychological distress significantly mediated the relationship between compulsivity and sleep quality (Table 4).
Diet quality and compulsivity
Figure 2 shows diet quality as a predictor of compulsivity is mediated by psychological distress. In Sample One, the total (c path; b = −0.5752, t(744) = −4.2317, P < .0001), direct (c΄ path; b = −0.3678, t(743) = −2.7383, P = .0063) and indirect (a and b paths multiplied; b = −0.2074, 95% CI = −0.3162 to −0.1157) effects of diet quality on compulsivity were significant. These results indicate that psychological distress partially mediated the relationship between diet quality and compulsivity, while diet quality maintained some direct influence on compulsivity after having accounted for distress.

Figure 2. Diet quality and compulsivity mediation models for Studies One (left) and Two (right). *Significant results at P < .05 level. **Significant results at P < .01 level. Solid lines indicate model where diet quality predicts compulsivity, mediated by distress Dashed lines indicate model where compulsivity predicts diet quality, mediated by distress.
Similarly in Sample Two, the total (c path; b = −0.4397, t(791) = −3.5821, P = .0004), direct (c΄ path; b = −0.2775, t(791) = −2.3788, P = .0176) and indirect (a and b paths multiplied; b = −0.1622, 95% CI = −0.2611 to −0.0743) effects of diet quality on compulsivity were significant replicating our interpretation of the data in Sample One wherein psychological distress partially mediated the relationship between diet quality and compulsivity.
When entering compulsivity as the predictor variable, we again found the relationship between the lifestyle factor and compulsivity to be bidirectional. Specifically, compulsivity significantly predicted diet quality, with psychological distress partially mediating this relationship (Table 4).
Physical activity and compulsivity
Across Studies One and Two, we found no significant total effect of MET minutes on compulsivity. We also found no significant total effect of compulsivity on MET minutes. Please refer to Figure 3 for an illustration of the relationship between MET minutes and compulsivity as mediated by psychological distress.

Figure 3. Physical activity and compulsivity mediation models for Studies One (left) and Two (right). *Significant results at the P < .01 level. **Significant results at the P < .05 level. Solid lines indicate model where physical activity predicts compulsivity, mediated by distress. Dashed lines indicate model where compulsivity predicts physical activity, mediated by distress.
Discussion
In this study, we gathered data from two large independent samples and undertook mediation analyses to examine the relationship between lifestyle factors and compulsivity, and whether this relationship is statistically explained by psychological distress. In particular, we focussed our investigation on the lifestyle factors of sleep quality, diet quality, and physical activity in separate mediation models. We found consistent results between the two samples. Our results showed an important role for psychological distress in explaining the bidirectional relationship between sleep quality and compulsivity, while psychological distress was somewhat important in explaining the bidirectional relationship between diet quality and compulsivity. Physical activity engagement did not predict compulsivity in either sample.
While some previous research has focused on the relationship between mental illness and lifestyle factorsReference Stubbs, Firth and Berry 56 - Reference Vancampfort, Firth and Schuch 58 including some compulsive disorders and lifestyle factors (for instance, OCD and its relationship with sleep,Reference Cox, Parmar and Olatunji 10 , Reference Segalàs, Labad and Salvat-Pujol 59 dietary intake in gambling disorder,Reference Chamberlain, Redden and Grant 11 and exercise for the treatment of OCDReference Abrantes, Farris and Brown 24 ), this is the first analysis—to our knowledge—of the relationship between lifestyle factors and transdiagnostic compulsivity. Our results therefore have important implications for both the prevention of compulsive disorders in vulnerable populations, early intervention in compulsive behaviors and the potential treatment of compulsive disorders through the initial target of psychological distress, and secondarily through lifestyle interventions.
Our results suggest that psychological distress, and building the individual’s resilience to distress, are important targets for psychological therapy interventions for compulsive disorders. Given that psychological distress is linked to compulsivity, the reduction of psychological distress may help to mitigate compulsive tendencies and behaviors. Psychological distress can be targeted through a range of existing first-line therapies including acceptance and commitment therapy and cognitive-behavioral interventions, particularly exposure and response prevention in this clinical group. Psychological distress may also be targeted through trained and self-led strategies such as mindfulness meditation. The practice of mindfulness meditation has been shown to increase the individual’s resilience to psychological distress when undertaken as a short and intensive intervention,Reference Ma, She, Siu, Zeng and Liu 60 , Reference Ostafin, Chawla, Bowen, Dillworth, Witkiewitz and Marlatt 61 as well as longer-term interventions with brief daily practice.Reference Grégoire and Lachance 62
Sleep and diet are both closely related to psychological distress,Reference Francis, Stevenson, Chambers, Gupta, Newey and Lim 34 - Reference Sadeghi, Keshteli, Afshar, Esmaillzadeh and Adibi 36 , Reference João, SND, Carmo and Pinto 39 and diet has been directly linked to compulsivity. The differences in these relationships may be explained through differing pathways. While evidence suggests that diet may directly impact on BDNF levelsReference Sánchez-Villegas, Galbete and Martinez-González 63 —a neurotrophic factor of which lower levels are associated with OCD,Reference Maina, Rosso, Zanardini, Bogetto, Gennarelli and Bocchio-Chiavetto 27 , Reference Wang, Mathews, Li, Lin and Xiao 28 , Reference Fontenelle, Guimarães Barbosa, Victor Luna, Pessoa Rocha, Silva Miranda and Lucio Teixeira 64 better sleep quality may improve resilience to psychological distress and emotion regulation which, in turn, may upregulate BDNF.Reference Schmitt, Holsboer-Trachsler and Eckert 32 , Reference Giese, Unternaehrer, Brand, Calabrese, Holsboer-Trachsler and Eckert 33 Our findings support a theory that two direct paths to BDNF involve diet and psychological distress, while sleep is involved through an indirect pathophysiological pathway.
Given the role of sleep and diet in psychological distress and the direct relationship between diet and compulsivity, lifestyle interventions appear to be prime candidates for inclusion in stepped models of holistic psychiatric care. The more widespread adoption of sleep and/or diet interventions to clinical practice may be beneficial for people who do not respond to treatments targeting psychological distress. They may also be effective in bolstering gains made through interventions targeting psychological distress. When assessing symptom changes during the course of a therapy or intervention, we suggest that it is important to monitor changes in psychological distress.
We found that physical activity, measured in MET minutes, had no significant relationship with compulsivity in either sample. Currently, there is mixed evidence on the links between physical activity and compulsive symptoms and behaviors, with weak evidence for its benefits.Reference Freedman and Richter 21 , Reference Okechukwu 65 Evidence from randomized controlled trials in OCD and substance use disorders suggests that planned and structured moderate- to high-intensity interval training may have the most profound impact on reducing compulsive behaviors and symptoms of compulsive disorders.Reference Abrantes, Farris and Brown 24 , Reference Wang, Wang, Wang, Li and Zhou 66 However, MET minutes may be seen as a crude measure of physical activity as includes low-, moderate-, and high-intensity activity without the total score distinguishing between these activities. Moreover, our measurement of physical activity—which includes the undertaking of incidental activities such as walking as a form of travelReference Caspersen, Powell and Christenson 67 —differs from existing research which suggests physical exercise—defined as planned and structured activity undertaken with the intention of improving physical fitnessReference Caspersen, Powell and Christenson 67 —should be a specific target for reducing compulsivity.
Our findings hold transdiagnostic importance and are pertinent to both clinical populations and populations as-risk of developing compulsive disorders. It may be the case that early interventions for subclinical groups that target the reduction of psychological distress or the improvement of diet and/or sleep quality will be an effective preventative measure to lower an individual’s risk of developing a clinical compulsive disorder, especially in people with high transdiagnostic compulsive tendencies. As individuals recover from compulsive disorders, interventions targeting psychological distress and lifestyle factors may be an effective, acceptable and low-cost means of preventing relapse and maintaining physical health, with the latter being associated with significant morbidity and mortality in those experiencing with mental health problems.Reference Firth, Siddiqi and Koyanagi 7
The current study is not without limitations. We undertook analyses on cross-sectional samples and employed self-report measures. This limits our ability to assess causal pathways, and data may be impacted by the accuracy of participants’ reports of their own lifestyle, psychological distress, and personality. We also conducted these studies in different countries during the COVID-19 pandemic. As health- socioeconomic- and cultural-related impacts of the pandemic were vastly different in Australia and the United States,Reference Bilinski and Emanuel 68 differential effects are likely to have impacted the factors we studied across these groups, including lifestyle. While previous research has indicated a relationship between psychological distress and lifestyle factors,Reference Li, Tian and Qin 69 , Reference Hinote, Cockerham and Abbott 70 we cannot necessarily generalize these results outside of Australia and the USA. Finally, we used different tools across studies to measure psychological distress and impulsivity. While we only used validated scales and our results suggest consistency across the two samples, it should be acknowledged that these tools may measure slightly different aspects of the same construct. For example, the S-UPPS-P measures the negative urgency aspect of impulsivity, while the BIS-11 does not. The K10 and DASS-21 also account for different psychological factors in the measure of psychological distress.
The current study has several strengths. We analyzed data from two large independent samples, which provide evidence of the reproducibility of the results. The current study and findings we have presented are novel, and yet to be documented in the existing empirical literature. Specifically, we looked at three lifestyle factors comprehensively and maintained a transdiagnostic approach in order to provide broad clinical utility of the results relevant to the general population, as well as a range of compulsive disorders. We analyzed samples across diverse socioeconomic and cultural population and found consistent links between lifestyle and compulsivity. The consistency of results between the samples reflects the study’s methodological rigor. Indeed, an advantage of conducting this study across countries with different outcomes from the COVID-19 pandemic illustrates that the relationship between lifestyle and compulsivity may be pervasive across cultures. Mediation analyses allowed us to provide further insight into these relationships through the important mediating factor of psychological distress which may be an important target for intervention, along with lifestyle interventions.
Conclusions
Looking ahead, there are a number of areas where research into the relationship between lifestyle factors and compulsivity/compulsive disorders may be required. Firstly, future research should investigate the aspects of diet which might be important to psychological distress and compulsivity such as adherence to a Mediterranean diet, or intake of particular noninflammatory foods, for example.Reference Willett, Sacks and Trichopoulou 71 Longitudinal studies assessing the aspects of lifestyle that lead to the transition to certain psychopathology will provide a clearer picture of the targets for patient education, early intervention and treatment for compulsive disorders. Future research may also focus more specifically on the measurement of high-intensity physical activity alone in order to focus the research toward understanding whether specific types of physical activity may reduce compulsive behaviors.
Funding Statement
M.E.B. is supported by an Australian Government Research Training Program (RTP) Scholarship. L.D. is supported by an Australian Government RTP Scholarship and a Monash Graduate Excellence Scholarship. S.R.C.’s research was funded by a Wellcome Clinical Fellowship (110049/Z/15/A and 110049/Z/15/Z). He previously consulted for Promentis and receives a stipend for editorial work at Elsevier. R.S.C.L. was funded by an NHMRC Investigator Grant from the Medical Research Future Fund (MRFF; #APP1193946). M.Y.’s role on this article was funded through a National Health and Medical Research Council Fellowship (NHMRC; #APP1117188). M.Y. also receives funding from other NHMRC schemes, Monash University, and Australian Government funding bodies such as the Australian Research Council (ARC), Australian Defence Science and Technology (DST), and the Department of Industry, Innovation and Science (DIIS). He has also received philanthropic donations from the David Winston Turner Endowment Fund, Wilson Foundation (which supported this study), as well as payments in relation to court-, expert witness-, and/or expert review-reports. L.F.F. is supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (# 302526/2018-8), Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (#E 26/203.052/2017), the D’Or Institute of Research and Education, and the David Winston Turner Endowment Fund. None of the above funding bodies were involved in the study design, management, data analysis and interpretation of results, or writing of the manuscript.
Disclosures
All authors have no conflicts of interest to declare.
Author Contributions
Conceptualization: M.E.B., L.A., K.R., M.Y., L.F.F.; Formal analysis: M.E.B., L.A., K.R., C.L., L.F.F.; Funding acquisition: M.Y.; Investigation: L.A.; Methodology: M.E.B., L.A., K.R., L.D., E.M.T., E.C., A.L., R.A.S., K.E.R., E.K., S.R.C., J.E.G., R.S.C.L., S.H., M.Y., L.F.F.; Project administration: M.E.B., L.A., K.R., E.M.T., E.C., A.L.; Supervision: L.A., L.F.F.; Writing—original draft: M.E.B.; Writing—review and editing: M.E.B., L.A., K.R., L.D., E.M.T., C.L., E.C., A.L., R.A.S., K.E.R., E.K., S.R.C., J.E.G., R.S.C.L., S.H., M.Y., L.F.F.
Supplementary Materials
To view supplementary material for this article, please visit http://doi.org/10.1017/S1092852921001048.









