Introduction
Inclusion body myositis is a sporadic, progressive, inflammatory myopathy characterised by asymmetric involvement of the quadriceps and finger flexors. Its incidence varies from 1.2 to 3.2 per million per year, and its prevalence is around 3–7 per 100 000 people.Reference Meyer, Meyer, Schaeffer, Gottenberg, Geny and Sibilia1 It is the most common myopathy after the age of 50 years.Reference Dimachkie and Barohn2 Unlike other inflammatory myopathies, and despite inflammatory histopathological findings, it is refractory to glucocorticoid treatment. Over time, it progresses to disability, which may contribute to increased mortality.Reference Cox, Titulaer, Sont, Wintzen, Verschuuren and Badrising3,Reference Price, Barghout, Benveniste, Christopher-Stine, Corbett and de Visser4
Dysphagia is reported as being a significant feature of inclusion body myositis, often being present at diagnosis.Reference Houser, Calabrese and Strome5 Estimates of dysphagia as a symptom range from 40 to 80 per cent of patients;Reference Mohannak, Pattison, Hird and Needham6–Reference Cox, Verschuuren, Verbist, Niks, Wintzen and Badrising8 however, this may be an underestimate of the problem.Reference Cox, Verschuuren, Verbist, Niks, Wintzen and Badrising8–Reference Schrey, Airas, Jokela and Pulkkinen10
The severity of dysphagia in inclusion body myositis can vary from mild to severe and is generally progressive over time. Even mild problems can have an impact on quality of life because of the limitations associated with social interaction, particularly around meals. There are also potential physical, social and psychological consequences.Reference Ekberg, Hamdy, Woisard, Wuttge-Hannig and Ortega11 As the dysphagia becomes more severe, it can result in a failure to maintain adequate nutrition, contributing to cachexia, and can give a predisposition to aspiration pneumonia. These factors are considered to contribute to mortality in patients with inclusion body myositis.Reference Cox, Titulaer, Sont, Wintzen, Verschuuren and Badrising3,Reference Capkun, Schmidt, Ghosh, Sharma, Obadia and de Vera12 Therefore, the diagnosis of dysphagia in this group and its subsequent assessment and treatment is important for the quality of life for patients with inclusion body myositis.
The aim of this review was to detail the presentation, assessment and treatment of patients with inclusion body myositis managed in the Oxford dysphagia clinic and review the findings with reference to the published literature.
Materials and methods
The aims, methods and results of this study were registered with the Ulysses Clinical Governance System (reference number: 6624) and approved by Oxford University Hospitals Foundation Trust.
The medical records of all patients with inclusion body myositis attending the Oxford dysphagia clinic between 2016 and 2020 were interrogated retrospectively. All patients were referred from the Oxford centre for neurology. The centre has a specialist interest in inclusion body myositis. All patients were referred with an established or suspected diagnosis of inclusion body myositis as well as swallowing difficulties and a desire to attend specialist services. All patients attending the clinic routinely completed the self-reported modified Sydney Swallow Questionnaire and the Reflux Symptom Index questionnaire (see Appendix 1).
All patients were jointly assessed by an ENT surgeon (author SW) and a speech and language therapist. Assessment included a comprehensive history and examination along with a range of clinical assessments including fibre-optic endoscopic evaluation of swallowing, with a range of textures and consistencies available.
Following clinical assessment, all patients received verbal and written advice regarding their swallowing. Additional assessments included video fluoroscopy or, on occasions, barium swallow. All imaging was assessed by two independent speech and language therapists and scored, where possible, using imaging features mentioned previously in the literature.Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13
All patients were treated with an advice-based approach initially and offered a follow up to assess their progress. Where appropriate, community-based speech and swallowing therapy was initiated with advice regarding the specifics of inclusion body myositis to support the community-based therapist.
Subsequent treatment was formulated through a discussion between the patient, speech and language therapist, and surgeon, utilising information from the self-reported questionnaires and investigations. This could involve further therapy and exercises, including advice about strategies to optimise safe swallow, pleasure while eating and adequate nutrition status. Treatment could also comprise balloon dilatation of the upper oesophageal sphincter, percutaneous feeding tube insertion, cricopharyngeal myotomy or botulinum toxin injection.
Where visualised data followed a normal distribution, mean and standard deviation were calculated; otherwise median and range were used. Correlation between questionnaires (ordinal data) was measured using Spearman's rank correlation coefficient.
Results
Between 2016 and 2020, 26 patients with inclusion body myositis were referred to the clinic. One patient was later found to be incorrectly diagnosed, and there were no available data for one patient; both were removed from analysis. Of the 24 patients included in this study, there were 13 male and 11 female patients. The mean age at first visit to the dysphagia clinic was 72 years (range, 54–84 years). For 4 patients (17 per cent), the diagnosis of inclusion body myositis was made while investigating their dysphagia symptoms. This included one patient who was investigated for dysphagia for eight years before eventually receiving a diagnosis of inclusion body myositis and being referred to the clinic.
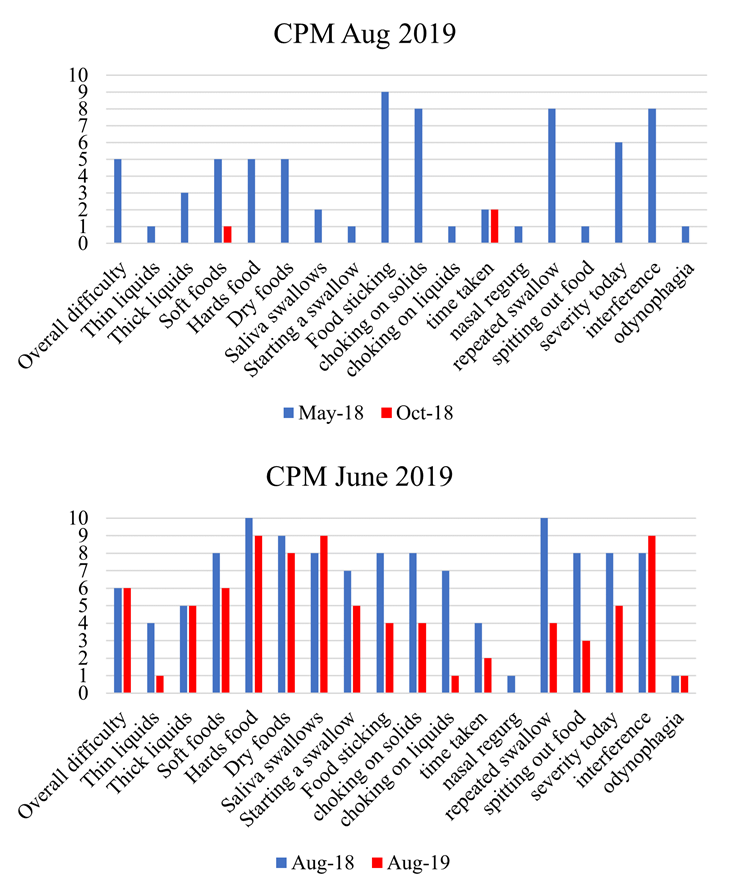
At their first visit to the clinic, 17 patients (71 per cent) completed baseline modified Sydney Swallow Questionnaire and Reflux Symptom Index questionnaire, and the remaining 6 patients completed these soon after. The mean and standard deviation of the total scores of the modified Sydney Swallow Questionnaire are 79 and 31 (range, 3–130; maximum possible score is 180). The profile of responses to the modified Sydney Swallow Questionnaire demonstrated a broad range (Figure 1). The symptoms that scored highest were problems with hard foods, food sticking, choking and repeated swallow. The symptoms that were least reported were odynophagia and nasal regurgitation.

Fig. 1. Results of the modified Sydney Swallow Questionnaires filled out at the initial presentation to the dysphagia clinic. The questions are displayed on the x-axis, with severity scored out of 10.
The results from the Reflux Symptom Index of all patients on their first presentation to the clinic demonstrated a mean score of 21 (range, 10–36; standard deviation, 7). Twenty-two of the 23 patients (96 per cent) for which we had results had a score above 13, suggesting that the reflux-related symptom burden is quite high in this cohort. All patients received written self-management advice, along with reflux medication where appropriate.
All patients underwent a contrast swallow assessment: 17 underwent video fluoroscopy and 7 underwent barium swallow for their first assessment. Barium swallows were initially performed at the inception of the clinic; they have been superseded by video fluoroscopy because of the higher image resolution and detail. All video swallows were performed with a speech and language therapist in attendance.
The baseline imaging features of the cohort upon presentation to the clinic are displayed in Table 1. The most prevalent features were impairment of tongue base retraction, residual pharyngeal pooling and pharyngeal constrictor impairment. Cricopharyngeal hypertrophy was found in 18 patients (75 per cent). Seven patients (30 per cent) had objective features of aspiration, with a median penetration aspiration score for the cohort of 2 (range, 1–8) (Figure 2).

Fig. 2. Penetration-aspiration scores (PAS) for the cohort. The worst score across all consistencies trialled was recorded. Median score was 2 and the range was 1–8.
Table 1. Imaging features

Table 1 displays features found on baseline video fluoroscopy or barium swallow on initial presentation to the clinic. Not all features could be scored from the imaging because of the frame rate of barium swallow, so there are variable denominators. All features were scored as binary presence or absence and were scored on fluid boluses only.
In order to see whether certain scales from the modified Sydney Swallow Questionnaire could ‘predict’ penetration-aspiration scaleReference Rosenbek, Robbins, Roecker, Coyle and Wood14 scores calculated on imaging, correlation coefficients were calculated. All questions had coefficients between −0.5 and +0.5 (data not presented).
All patients received targeted speech and swallowing advice and were offered a review appointment, either remotely or face-to-face. Sixteen patients (67 per cent) returned to clinic for review. All patients had the option of being followed up by the community speech and language teams.
Sixteen patients (67 per cent) in the cohort received swallowing advice but no surgical intervention; we followed them up over time. Three patients (13 per cent) completed repeat modified Sydney Swallow Questionnaires a few months after being given the swallowing advice; their serial scores were largely quite similar, despite reporting their dysphagia to be improved overall.
Four patients (17 per cent) in this group had serial video swallows over the course of several years, which allows us to see the natural progression of dysphagia in inclusion body myositis. These limited data show increasing penetration-aspiration scale scores and impairment over time (data not shown).
Six patients (25 per cent) received active surgical intervention. Three received more than one different procedure: oesophageal dilatation (performed in 4 patients), radiologically inserted percutaneous gastrostomy (1 patient), cricopharyngeal myotomy (2 patients) and botulinum toxin injection to the cricopharyngeus muscle (1 patient).
The effect of the different procedures was measured by serial modified Sydney Swallow Questionnaire. Given the low numbers, data have not been presented or statistically analysed but are briefly described here. Balloon dilatation was offered to patients with cricopharyngeal hypertrophy on contrast swallow and symptomatic obstruction. Of the four patients in this group, only one derived lasting benefit from a single dilatation. The other three either derived no benefit or experienced a recurrence in their symptoms: one went on to have two repeat dilatations (the last with botulinum toxin injection to the cricopharyngeus muscle) without benefit; one patient improved after radiologically inserted percutaneous gastrostomy insertion; and one patient only benefited from a cricopharyngeal myotomy. Cricopharyngeal myotomy was offered to two patients based on imaging features and severity of dysphagia; both reported subjective improvement in their swallow (Figure 1 in the supplementary material, available on The Journal of Laryngology & Otology website).
Discussion
Patients in our cohort were referred to the clinic because of concerns over dysphagia. They therefore represent a subset of inclusion body myositis patients encountered in clinical practice. Subtle features of dysphagia in inclusion body myositis may be present without spontaneous reporting: in a study by Cox et al.,Reference Cox, Verschuuren, Verbist, Niks, Wintzen and Badrising8 37 of 57 patients had symptoms of dysphagia picked up by a questionnaire, but only 17 spontaneously reported dysphagia during clinical assessment.
The patients in our cohort were almost evenly split between the sexes: 13 male and 11 female. This is an interesting finding given that other studies have found that the majority of patients with inclusion body myositis are male.Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13,Reference Phillips, Zilko and Mastaglia15 The mean age at presentation is comparable with other studies.Reference Cox, Verschuuren, Verbist, Niks, Wintzen and Badrising8,Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13 One patient in our study died because of aspiration pneumonia, though our patients were only followed up over the four-year study duration.
Four patients (17 per cent) had dysphagia as their presenting symptom of inclusion body myositis; this is unusual since dysphagia is thought to usually present later in the disease.Reference Cox, Verschuuren, Verbist, Niks, Wintzen and Badrising8,Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13,Reference Badrising, Maat-Schieman, van Houwelingen, van Doorn, van Duinen and van Engelen16,Reference Lotz, Engel, Nishino, Stevens and Litchy17 One patient in our cohort was investigated for dysphagia for eight years before their diagnosis of inclusion body myositis, similar to a previous case report.Reference Shibata, Izumi, Hara, Ohshima, Nakamura and Suzuki18
Twenty-three patients presenting to our clinic completed a Reflux Symptom Index questionnaire. The median score was 21. Normative data suggests that a Reflux Symptom Index score greater than 13 may be indicative of significant reflux. Twenty-two patients (96 per cent) had scores over 13, suggesting this could be a common component of the symptom burden. When reflux was identified, this was addressed with discussion, written advice and provision of reflux medication. However, the Reflux Symptom Index has not been correlated with reflux in an inclusion body myositis population. It is therefore possible that the high score reflects the underlying dysphagia associated with inclusion body myositis. Additional studies would be needed to evaluate the correlation of the Reflux Symptom Index in this population.
Results from the cohort's modified Sydney Swallow Questionnaires suggest particular difficulties with hard and dry food, food sticking, and repeated swallowing. These results resemble those found previously in the literature,Reference Mulcahy, Langdon and Mastaglia7,Reference Cox, Verschuuren, Verbist, Niks, Wintzen and Badrising8,Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13 suggesting these are common features of the dysphagia in inclusion body myositis. These questions could provide a good screening for dysphagia in these patients.
All patients underwent contrast swallow assessment (Figure 3 and Table 1). The most common features identified were impairment in tongue base retraction (96 per cent), pharyngeal constriction (82 per cent) and residual pharyngeal pooling (92 per cent). Cricopharyngeal dysfunction and hypertrophy were identified in 75 per cent of patients, a figure comparable with previous studies.Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13 Aspiration was identified in 30 per cent of patients at baseline. Median penetration-aspiration score was 2, similar to a previous study,Reference Murata, Kouda, Tajima and Kondo9 although the distribution of scores was uneven (Figure 2). However, it should be noted that we did not have a standardised protocol to ensure inter-rater reliability, nor any software to measure dynamics of upper oesophageal sphincter opening. Moreover, barium swallows have a lower frame per second rate and quality compared with videofluoroscopy. Therefore, we recommend that future studies use videofluoroscopy to better define swallowing abnormalities and that there is a validated protocol and analysis tool (e.g. the Modified Barium Swallow Impairment Profile). Given the reported difficulties with solids, incorporating both fluid and solid boluses within the video fluoroscopy protocol could be informative for this population.

Fig. 3. Images of video fluoroscopy showing common features identified. (a) Sagittal view of cricopharyngeal hypertrophy evident at the height of swallow (maximal displacement of the hyoid), (b) sagittal view of silent aspiration of post-swallow pharyngeal residue, (c) coronal view of spontaneous, passive opening of the cricopharyngeus muscle to allow eventual bolus transit into the oesophagus and (d) sagittal view of cricopharyngeal hypertrophy and laryngeal penetration evidence at the height of swallow (maximal displacement of the hyoid).
• This study described a UK cohort of patients with inclusion body myositis, presenting with dysphagia to a tertiary centre
• The reflux symptom index suggested an issue with significant reflux in these patients, something not previously realised
• Swallow questionnaires and imaging showed common problems with swallowing amongst these patients
• Many patients can be managed by community speech and language teams, but should be assessed by a specialised service for possible operative intervention
All patients received support by our speech and language team. This support depended on several factors: the swallow mechanism, risks associated with oral intake, imaging results, patient goals and effect on life. The amount and timing of therapy was tailored to individual need.
Six of our patients (25 per cent) underwent surgical procedures, a lower proportion than in previous studies.Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13 Three of the four who underwent balloon dilatation received no lasting benefit and required further procedures. These findings are similar to those of Oh et al. (2008), who found that the majority of dilatations resulted in no benefit.Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13
Only one patient received botulinum toxin injection to alleviate their dysphagia; symptoms improved for just one month before recurrence. By contrast, some studies have shown longer lasting benefits,Reference Schrey, Airas, Jokela and Pulkkinen10,Reference Liu, Tarnopolsky and Armstrong19 whereas others have suggested limited efficacy.Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13
Cricopharyngeal myotomy was only offered to three patients in our cohort and was performed in two patients; it was effective at improving dysphagia in both without documented complications. Cricopharyngeal myotomy was reported to be an effective procedure in several previous studies when used appropriately, using either an endoscopic or transcervical approach.Reference Houser, Calabrese and Strome5,Reference Mohannak, Pattison, Hird and Needham6,Reference Oh, Brumfield, Hoskin, Kasperbauer and Basford13,Reference Langdon, Mulcahy, Shepherd, Low and Mastaglia20,Reference McMillan, Bowen, Bayan, Kasperbauer and Ekbom21
There were several limitations to this study. There was a small sample size, but inclusion body myositis is a rare condition. The study was retrospective and there was limited follow up for a few patients who were most recently referred. However, despite these limitations, we recommend that all patients with inclusion body myositis and dysphagia undertake serial modified Sydney Swallow Questionnaires and videofluoroscopy in order to fully assess their dysphagia and to quantify the effect of the different interventions. Moreover, the high reporting of reflux symptoms suggested that actively screening and treating reflux at an early stage should be considered. Future research should include the use of validated swallowing scales such as the Modified Barium Swallow Impairment ProfileReference Martin-Harris, Brodsky, Michel, Castell, Schleicher and Sandidge22 to allow for standardised analysis of swallow features alongside the use of additional outcome measures such as the penetration aspiration scaleReference Steele and Grace-Martin23 and the Dynamic Imaging Grade of Swallowing Toxicity measureReference Hutcheson, Barrow, Barringer, Knott, Lin and Weber24 to detail residue, penetration and aspiration.
Conclusion
This study helps to profile features of dysphagia in patients with inclusion body myositis, both subjectively (via questionnaires) and objectively (contrast imaging). We described progression of dysphagia in inclusion body myositis in a cohort of our patients and described our practice. We outlined suggestions on how to improve the quality of research in this area. More work is needed on these patients in order to better evaluate common symptoms, imaging features and management strategies and perform relevant statistical analysis.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0022215121004758.
Data availability statement
All data are available on request.
Competing interests
None declared
Appendix 1. Modified Sydney Swallow Questionnaire
Visual Analogue Scale. Each question is measured out of 10.
1. How much difficulty do you have swallowing at present?
No difficulty at all |--------------------------------| Unable to swallow at all.
2. How much difficulty do you have swallowing THIN liquids (e.g. tea, soft drink, beer, coffee)?
No difficulty at all |--------------------------------| Unable to swallow at all.
3. How much difficulty do you have swallowing THICK liquids (e.g. milkshakes, soups, custard)?
No difficulty at all |--------------------------------| Unable to swallow at all.
4. How much difficulty do you have swallowing SOFT foods (e.g. mornays, scrambled eggs, mashed potatoes)?
No difficulty at all |--------------------------------| Unable to swallow at all.
5. How much difficulty do you have swallowing HARD foods (e.g. steak, raw fruit, raw vegetables)?
No difficulty at all |--------------------------------| Unable to swallow at all.
6. How much difficulty do you have swallowing DRY foods (e.g. bread, biscuits, nuts)?
No difficulty at all |-------------------------------| Unable to swallow at all.
7. Do you have any difficulty swallowing your own saliva?
No difficulty at all |-------------------------------| Unable to swallow at all.
8. Do you have any difficulty starting a swallow?
Never occurs |---------------------------------| Occurs every time I swallow.
9. Do you ever have a feeling of food getting stuck in your throat when you swallow?
Never occurs |----------------------------------| Occurs every time I swallow.
10. Do you ever cough or choke when swallowing solid foods (e.g. bread, meat or fruit)?
Never occurs |---------------------------------| Occurs every time I swallow.
11. Do you ever cough or choke when swallowing liquids (e.g. coffee, tea, water, beer)?
Never occurs |---------------------------------| Occurs every time I swallow.
12. How long does it take you to eat an average meal? Please tick one.
Less than 15 minutes (scored 0)
About 15–30 minutes (scored 2)
About 30–45 minutes (scored 4)
About 45–60 minutes (scored 6)
More than 60 minutes (scored 8)
Unable to swallow at all (scored 10)
13. When you swallow, does food or liquid go up behind your nose or come out your nose?
Never occurs |---------------------------------| Occurs every time I swallow.
14. Do you ever need to swallow more than once for your food to go down?
Never occurs |---------------------------------| Occurs every time I swallow.
15. Do you ever cough up or spit out food or liquids DURING a meal?
Never occurs |---------------------------------| Occurs every time I swallow.
16. How do you rate the severity of your swallowing problem today?
No problem |-------------------------------------| Extremely severe problem.
17. How much does your swallowing problem interfere with your enjoyment or quality of life?
No interference |---------------------------------------| Extreme interference.
18. How painful is it to swallow?
Not at all |---------------------------------------------------------| Very painful.
The Reflux Symptom Index
Within the last month, how did the following problems affect you?
(0–5 rating scale with 0 = No problem and 5 = Severe)
Normative data suggests that a Reflux Symptom Index of greater than or equal to 13 is clinically significant. Therefore a Reflux Symptom Index >13 may be indicative of significant reflux disease.
1. Hoarseness or a problem with your voice
0 1 2 3 4 5
2. Clearing your throat
0 1 2 3 4 5
3. Excess throat mucous or postnasal drip
0 1 2 3 4 5
4. Difficulty swallowing food, liquids, or pills
0 1 2 3 4 5
5. Coughing after you ate or after lying down
0 1 2 3 4 5
6. Breathing difficulties or choking episodes
0 1 2 3 4 5
7. Troublesome or annoying cough
0 1 2 3 4 5
8. Sensations or something sticking in your throat
0 1 2 3 4 5
9. Heart burn, chest pain, indigestion, or stomach acid coming up
0 1 2 3 4 5