



Introduction
Anxiety and mood disorders are among the most prevalent mental health problems faced by our growing population of older adults worldwide. Research using nationally representative data from the United States of America and Canada has shown that between 3 and 7 per cent of older adults meet clinical diagnostic criteria for any past-year mood disorder, and between 3 and 11 per cent of older adults meet criteria for any past-year anxiety disorder (Scott et al., Reference Scott, MacKenzie, Chipperfield and Sareen2010; Reynolds et al., Reference Reynolds, Pietrzak, El-Gabalawy, Mackenzie and Sareen2015). Systematic reviews and meta-analytic studies indicate global prevalence estimates of major depression ranging from 1 to 5 per cent among adults 65 years and older (Alexopoulos, Reference Alexopoulos2005; Djernes, Reference Djernes2006; Sutin et al., Reference Sutin, Terracciano, Milaneschi, An, Ferrucci and Zonderman2013; Purtle et al., Reference Purtle, Nelson, Yang, Langellier, Stankov and Diez Roux2019). Prevalence estimates of sub-threshold depressive symptoms are approximately two to three times higher than clinical diagnoses of major depressive disorder among adults aged 65 years and older, with global estimates of 15 per cent of older adults experiencing clinically significant depressive symptoms in the absence of meeting full diagnostic criteria (Meeks et al., Reference Meeks, Vahia, Lavretsky, Kulkarni and Jeste2011). Studies estimate that 8–10 per cent of older adults with sub-threshold depressive symptoms develop major depression within a year (Meeks et al., Reference Meeks, Vahia, Lavretsky, Kulkarni and Jeste2011). Depressive symptoms among older adults have been highlighted as a public health priority due to the significant risk of poor outcomes associated with depression, including physical health problems; suicide; mortality; and reduced physical, cognitive and social functioning (Purtle et al., Reference Purtle, Nelson, Yang, Langellier, Stankov and Diez Roux2019).
Although effective treatment options for late-life stress, anxiety and mood disorders exist (e.g. Wetherell et al., Reference Wetherell, Lenze and Stanley2005; Ayers et al., Reference Ayers, Sorrell, Thorp and Wetherell2007; Karlin and Fuller, Reference Karlin and Fuller2007; Andreescu and Reynolds, Reference Andreescu and Reynolds2011; Payman, Reference Payman2011; Hunsley et al., Reference Hunsley, Elliott and Therrien2014), as many as 70 per cent of older adults with mood and anxiety disorders do not utilise services (Byers et al., Reference Byers, Arean and Yaffe2012). Qualitative research exploring older adults’ narratives of seeking mental health treatment highlights the nuanced and complex pathways to treatment for older adults (Reynolds et al., Reference Reynolds, Medved, Mackenzie, Funk and Koven2020). Three main storylines emerged in this qualitative analysis, including: resistance to being labelled with mental health problems; muddling through the help-seeking process; and emotional reactions to psychological treatment. In the second storyline, older adults’ muddling through the treatment-seeking process illustrated a system-induced passivity, neither resisting nor actively seeking out psychological treatment, and traversing from one referral or treatment option to the next. This type of system-induced passivity may have been brought about by limited knowledge about mental health and related treatment services, and few options for shared decision-making with health-care providers (Reynolds et al., Reference Reynolds, Medved, Mackenzie, Funk and Koven2020). In light of elevated rates of mental health problems and low rates of psychological help-seeking among older adults, the current study sought to describe the mental health information preferences and predictors of preferences among a sample of older adults residing in central Canada. In the sections that follow, we provide contextual information concerning the importance of mental health literacy and shared decision-making surrounding mental health treatment, and the gaps within these important research areas.
There is growing support in the literature that inadequate mental health literacy, defined as knowledge and beliefs about mental disorders, their recognition, management or prevention, can be a barrier to service use among older adults (Jorm et al., Reference Jorm, Korten, Jacomb, Christensen, Rodgers and Pollitt1997; Fisher and Goldney, Reference Fisher and Goldney2003; Farrer et al., Reference Farrer, Leach, Griffiths, Christensen and Jorm2008; Wetherell et al., Reference Wetherell, Petkus, McChesney, Stein, Judd, Rockwell, Sewell and Patterson2009; Jorm, Reference Jorm2012; Kim et al., Reference Kim, Rhee, Lee, Park and Sharratt2017; Nakash et al., Reference Nakash, Hayat, Abu Kaf and Cohen2020). Older adults’ rates of mental health literacy are significantly lower relative to younger adults, with research showing that older adults make more errors in recognising mental health problems including anxiety, depression and schizophrenia. Compared to younger age groups, older adults are also less likely to recommend that individuals with mental health problems seek professional help (Fisher and Goldney, Reference Fisher and Goldney2003; Farrer et al., Reference Farrer, Leach, Griffiths, Christensen and Jorm2008; Wetherell et al., Reference Wetherell, Petkus, McChesney, Stein, Judd, Rockwell, Sewell and Patterson2009). Evidence suggests that interventions (i.e. Mental Health First Aid), community campaigns and internet websites targeting the provision of mental health knowledge (recognition and management) to the public can increase mental health literacy (Jorm, Reference Jorm2012; Kim et al., Reference Kim, Rhee, Lee, Park and Sharratt2017). These interventions and informational resources, if appropriately targeted towards unique factors associated with age and culture, could help to inform shared decision-making concerning mental health treatments (Kim et al., Reference Kim, Rhee, Lee, Park and Sharratt2017).
Researchers have begun to demonstrate that although older adults express a desire to be involved in their health-care decision-making (i.e. treatment decisions), they are often not given sufficient information to participate in this process (O'Neal et al., Reference O'Neal, Adams, McHugo, Van Citters, Drake and Bartels2008; Chiu et al., Reference Chiu, Feuz, McMahan, Miao and Sudore2016; Gonzalez et al., Reference Gonzalez2019). Providing information to the public/patients prior to making decisions concerning mental health treatment and supports leads to increased understanding and recall of information, as well as patient satisfaction and compliance with treatment (Faden et al., Reference Faden, Becker, Lewis, Freeman and Faden1981; Deyo and Diehl, Reference Deyo and Diehl1986; Hall et al., Reference Hall, Roter and Katz1988; Shen et al., Reference Shen, Manna, Banerjee, Nelson, Alexander, Alici, Gangai, Parker and Korc-Grodzicki2020). Unfortunately, patients often receive less information than they desire and the information that they do receive can be inadequate for addressing their needs (Boreham and Gibson, Reference Boreham and Gibson1978; Jenkins et al., Reference Jenkins, Fallowfield and Saul2001; Boberg et al., Reference Boberg, Gustafson, Hawkins, Offord, Koch, Wen, Kreutz and Salner2003; Rogers et al., Reference Rogers, Kennedy, Nelson and Robinson2005). This finding is especially problematic for older adults, who report a preference to be involved in decision-making concerning health treatment options (O'Neal et al., Reference O'Neal, Adams, McHugo, Van Citters, Drake and Bartels2008; Chiu et al., Reference Chiu, Feuz, McMahan, Miao and Sudore2016; MacRae, Reference MacRae2018). Qualitative research by MacRae (Reference MacRae2018) explored older Canadian women's beliefs concerning their interactions with physicians, with the aim of furthering understanding of the experience of ageism and sexism in the primary medical care of older women. Analyses revealed that while both ageism and sexism were present in the experiences of older women, ageism was pronounced. One theme highlighted women's perceptions that physicians preferred younger patients. For example, one participant noted: ‘I suspect they take a more active interest in younger patients. They may kind of write you off as, it's all in your head.’ Another described, ‘There are doctors who don't want elderly patients because they take more time’ (MacRae, Reference MacRae2018: 247).
Although extant research on information preferences is limited, findings indicate that adults with mental health problems and their families have many information needs that remain unaddressed (Buckland, Reference Buckland1994; Cleary et al., Reference Cleary, Freeman, Hunt and Walter2005; Drapalski et al., Reference Drapalski, Marshall, Seybolt, Medoff, Peer, Leith and Dixon2008; Fossey et al., Reference Fossey, Harvey, Mokhtari and Meadows2012; Burns et al., Reference Burns, Da Silva and John2021). The unmet information needs of older adults include information about mental health problems, outcomes of mental health problems, treatment options and individual treatment progress (Fossey et al., Reference Fossey, Harvey, Mokhtari and Meadows2012). Inpatient and outpatient young- to middle-aged adults with mental health problems, as well as their care-givers, desire enhanced information, preferring knowledge on: steps to take if feeling unwell; information about medication treatment; knowledge about the ways in which others cope with similar mental health problems; and information about mental health services in the community (Cleary et al., Reference Cleary, Freeman, Hunt and Walter2005). A recent systematic review exploring shared decision-making preferences in mental health highlighted older adults’ desire for involvement in mental health-related treatment decisions (Burns et al., Reference Burns, Da Silva and John2021). Conclusions prompted a call for more ‘high-quality research regarding the shared decision-making preferences and outcomes of older adults with mental ill-health’ (Burns et al., Reference Burns, Da Silva and John2021: 634).
As indicated above, systemic patterns of ageism may underlie the reasons for which older adults are not given ample opportunity to participate in shared decision-making within health care (MacRae et al., Reference MacRae2018). Ageist medical practices, including lack of shared decision-making, may highlight remnants of a deficit-model of thinking, whereby the later stage of life is portrayed as the phase of rest, dependency and decline. Researchers posit that current policies and practices regarding older adults’ involvement in shared decision-making are outdated and are not in line with updated thinking around active ageing and competence theories put forth over the past two to three decades (Jacobs, Reference Jacobs2005; Boudiny, Reference Boudiny2013).
Specific mental health information preferences among older adults remain unknown, and are in need of exploration, particularly in light of recent calls in the literature (Burns et al., Reference Burns, Da Silva and John2021). There is an absence of research examining preferences for amount (how much information they would want), format (in what format they would like to receive this information) and source (from whom they would like to access this information) of mental health information.
Further to this, there is a gap in knowledge concerning predictors of mental health information preferences of older adults. Although this topic has not been explored with regard to mental health and older adults, it has been examined among cancer populations. Findings in this research area indicate that preferences for greater amounts of health information are associated with younger age (Galarce et al., Reference Galarce, Ramanadhan, Weeks, Schneider, Gray and Viswanath2011), higher educational attainment (Galarce et al., Reference Galarce, Ramanadhan, Weeks, Schneider, Gray and Viswanath2011), non-White race (Beckjord et al., Reference Beckjord, Arora, McLaughlin, Oakley-Girvan, Hamilton and Hesse2008), female sex (Neame et al., Reference Neame, Hammond and Deighton2005), comorbid health problems (Beckjord et al., Reference Beckjord, Arora, McLaughlin, Oakley-Girvan, Hamilton and Hesse2008), decreased perception of physical and mental health status (Beckjord et al., Reference Beckjord, Arora, McLaughlin, Oakley-Girvan, Hamilton and Hesse2008), higher psychological distress (Stewart et al., Reference Stewart, Wong, Cheung, Dancey, Meana, Cameron, McAndrews, Bunston, Murphy and Rosen2000) and higher levels of social support (Askelson et al., Reference Askelson, Campo and Carter2011). Knowing older adults’ mental health information preferences and socio-demographic and psycho-social predictors of these preferences will help to tailor mental health information to older adults, with ultimate aims of improving mental health literacy and enhancing empowerment in mental health help-seeking.
Objectives
The objectives of this study were to describe the mental health information preferences of older adults and determine the socio-demographic and psycho-social predictors of their mental health information preferences. We hypothesised that socio-demographic and psycho-social characteristics would be associated with older adults’ mental health information preferences. Specifically, in line with prior research examining health information preferences among cancer populations, we expected that information preferences (i.e. content, amount, format and source) would be associated with younger age, higher educational attainment, non-White race, female sex, comorbid health problems, decreased perception of physical and mental health status, greater psychological distress, more favourable attitudes towards treatment and greater levels of social support.
Method
Participants and recruitment
We received Institutional Review Ethics Board approval prior to recruitment and data collection. We recruited adults ages 50 years and older through senior centres (N = 127) and primary care clinics (N = 102) in central Canada from September 2013 to April 2014 (total N = 229). The response rate for participants recruited from medical clinics was 74 per cent, with participants declining to participate due to various reasons, including not feeling well, perceived insufficient English-language proficiency, print too small to see without glasses and insufficient time to participate. We were not able to assess the response rate for senior centre participation, though all participants who were invited to senior centre events to participate in this research completed the survey. Participants received a Can $5 gift card to a coffee shop as an honorarium for their involvement.
Measures
Mental health information questionnaire
Participants completed the mental health information questionnaire in their primary care clinic or senior centre in paper-based format, which consisted of a battery of questions investigating socio-demographic, psycho-social and health-related characteristics, as well as mental health information preferences. In order to ensure the reliability and validity of participant ratings, we constructed items with five-point response options, which are accompanied by a numerical and verbal label (Krosnick and Presser, Reference Krosnick, Presser, Wright and Marsden2010). The socio-demographic information in the questionnaire included: age, sex, race/ethnicity, marital status, education, current occupation and annual household income. Measurement of psycho-social characteristics consisted of the six-item Kessler Psychological Distress measure (K6; Kessler et al., Reference Kessler, Andrews, Colpe, Hiripi, Mroczek, Normand, Walters and Zaslavsky2002), the six-item version of the Lubben Social Network Scale (LSNS-6; Lubben et al., Reference Lubben, Blozik, Gillmann, Iliffe, von Renteln Kruse, Beck and Stuck2006) and the Attitudes Toward Seeking Professional Psychological Help Scale – Short Form (ATSPPHS-SF; Fischer and Farina, Reference Fischer and Farina1995). Health-related characteristics included questions pertaining to self-rated mental and physical health and personal experience with mental health problems and treatment, and were based on questions from the Canadian Community Health Survey (Statistics Canada, 2002) as well as research conducted by the Mobilizing Minds Research Group (Stewart et al., Reference Stewart, Walker, Beatie, Reynolds, Hahlweg, Leonhart and Tulloch2014). Participants began by completing a consent form followed by the mental health information questionnaire. On average, participants completed the questionnaire in 27.5 minutes, with completion times ranging from 15 to 40 minutes.
Kessler Psychological Distress measure (K6)
The K6 is a six-item self-report scale that measures feelings of distress over the past 30 days on a five-point rating scale with response options ranging from 0 (none of the time) to 4 (all of the time) (Kessler et al., Reference Kessler, Andrews, Colpe, Hiripi, Mroczek, Normand, Walters and Zaslavsky2002). Scores range from 0 to 24, with higher scores indicating greater distress, and a cut point of ⩾5 on the K6 to identify those with moderate mental distress (Prochaska et al., Reference Prochaska, Sung, Max, Shi and Ong2012). Previous research has demonstrated that the K6 has good internal consistency (Kessler et al., Reference Kessler, Andrews, Colpe, Hiripi, Mroczek, Normand, Walters and Zaslavsky2002; α = 0.89), which was also shown with the current sample (α = 0.85).
Lubben Social Network Scale (LSNS-6)
Participants completed the LSNS-6, which measures social isolation and social support/connectedness on a five-point rating scale. Questions on the LSNS-6 address how many relatives/friends one is in contact with approximately once a month, how many relatives/friends one feels close to and how many relatives/friends one feels at ease with to talk about private matters. Response options range from 1 to 9+, with total scores ranging from 6 to 30. Higher scores represent greater social connectivity, and a cut point of <12.0 represents social isolation/loneliness (Lubben et al., Reference Lubben, Blozik, Gillmann, Iliffe, von Renteln Kruse, Beck and Stuck2006). This scale has good internal consistency (α = 0.83) and adequate test–retest reliability (κ = 0.64) (Lubben et al., Reference Lubben, Blozik, Gillmann, Iliffe, von Renteln Kruse, Beck and Stuck2006). Good internal consistency of the LSNS-6 was also demonstrated with the current sample (α = 0.83).
Attitudes Toward Seeking Professional Psychological Help Scale – Short Form (ATSPPHS-SF)
Participants completed the ten-item ATSPPHS-SF as a measure of attitudes towards seeking mental health care (Fischer and Farina, Reference Fischer and Farina1995). When completing the ATSPPHS-SF, participants responded to items on a four-point rating scale, with response options ranging from 0 (disagree) to 3 (agree). Total scores range from 0 to 30, with higher scores representing more favourable attitudes towards mental health treatment. The ATSPPHS-SF has adequate internal consistency (α = 0.77–0.78) and good test–retest reliability (r = 0.80) (Fischer and Farina, Reference Fischer and Farina1995; Komiya et al., Reference Komiya, Good and Sherrod2000; Constantine, Reference Constantine2002; Vogel et al., Reference Vogel, Wester, Wei and Boysen2005; Elhai et al., Reference Elhai, Schweinle and Anderson2008; Hunsley and Mash, Reference Hunsley and Mash2008). Adequate internal consistency was also demonstrated with the current sample (α = 0.77).
Mental health information preferences
Prior to answering questions examining mental health information preferences (i.e. content, amount, format and source), participants read a vignette, tailored to their respective sex, which described the experience of an older adult with major depression. Participants read this vignette in order to promote their ability to recognise that the older adult had a problem and understand the problem as depression. Research demonstrates older adults are more likely to recognise the symptoms of depression, as compared to the symptoms of anxiety (Wetherell et al., Reference Wetherell, Petkus, McChesney, Stein, Judd, Rockwell, Sewell and Patterson2009). Furthermore, research has shown that older adults are more likely to identify depression correctly when there is information pertaining to sadness in addition to somatic symptoms such as loss of appetite and disruptions in sleep (Wetherell et al., Reference Wetherell, Petkus, McChesney, Stein, Judd, Rockwell, Sewell and Patterson2009; Gum et al., Reference Gum, McDougal, McIlvane and Mingo2010). In light of these findings, we chose depression as the mental health problem and included somatic symptoms. Participants endorsed their preferences for mental health information (content, amount, format and source) on five-point rating scales. Vignettes were developed based on the clinical expertise of the research team (article authors), in line with prior vignettes developed by researchers in the area of mental health literacy (Morgan et al., Reference Morgan, Reavley and Jorm2014).
Content
Within the content section of the questionnaire, participants began by indicating their level of familiarity with the types of professional help available for mental health problems (e.g. stress, anxiety, depression). After completing this question, participants responded to questions concerning their perceptions of the importance of a variety of mental health information content on a five-point rating scale with response options ranging from 1 (not at all important) to 5 (critical). Participants were also prompted to identify other information they would like to know before deciding about seeking help for a mental health problem.
Amount
When answering questions pertaining to their preferred amount of information, participants indicated the quantity of information that they would prefer concerning medication treatment, counselling or psychological treatment, combined medication and psychological treatment, and self-help approaches. Participants responded on a five-point rating scale with response options ranging from ‘no information at all’ to ‘moderate information’ (brief pamphlet or one-page fact sheet) to ‘detailed information’ (two to six pages).
Format
With regard to the format of information, participants responded to questions concerning their preferences of written information, information received through discussion with a heath-care provider, information provided in the form of a DVD, or information on a recommended internet website. In this section, participants responded on a five-point rating scale with response options ranging from 1 (not preferred) to 5 (extremely preferred). This section of the mental health questionnaire also contained a question asking participants to identify other information formats that they would find helpful if they were experiencing a mental health problem and looking for help.
Source
Participants responded to questions examining the sources that they would be likely to contact should they experience a mental health problem. Sources of information presented in the questionnaire included: spouse or romantic partner, child/children, sibling(s), close friend(s), family doctor, mental health professional, pharmacist, community newspaper, recommended self-help book, or an internet website or discussion group. Participants responded to these questions on a five-point rating scale with response options ranging from 1 (not at all likely) to 5 (extremely likely), with an additional ‘not applicable’ response option. The mental health questionnaire concluded with a question prompting participants to identify additional sources they would consult if experiencing a mental health problem and seeking help.
Analyses
Results of a missing-values analysis indicated 98 per cent complete values in the dataset, with an absence of clear patterns to the missing data (Little's MCAR chi-square = 1,413.0, p > 0.05). In a missing-value analysis, we used expectation maximisation with 25 iterations. Multiple imputation method (with five imputations) on missing data resulted in imputed values for age, education, household income and marital status. All other variables were not imputed due to no or too few missing values. When comparing regression coefficients (R 2 and ΔR 2) of the imputed and original datasets, there were similar values and identical patterns in the data. As such, all analyses are presented using the original dataset.
Mental health information preferences
We analysed findings with the total sample of older adults, keeping age as a continuous variable. To address the first study objective (describe the mental health information preferences of older adults), we conducted descriptive analyses to quantify older adults’ ratings of information preferences according to three levels, recoded from the initial five-level scale responses. Our decision to collapse response options was based on the large volume of data and desire to present information in a way that enhances readability and interpretability. We also calculated the mean rating and 95 per cent confidence interval for each information preference item. We conducted principal components analysis (PCA) on the information preference variables, in order to condense items for descriptive tables as well as reduce the number of variables to use in subsequent regression analyses. Decisions concerning number of factors to retain centred upon visual inspection of the scree plot, retaining factors in the steep curve before the line trends downwards or levels off (Courtney, Reference Courtney2013).
Predictors of mental health information preferences
To address the second study objective (to determine the socio-demographic and psycho-social predictors of older adults’ mental health information preferences), we conducted hierarchical linear regression analyses with socio-demographic and psycho-social characteristics as independent variables predicting the dependent variables (information preferences). For each regression analysis, we entered socio-demographic variables in step 1 (i.e. sex, race/ethnicity, age, education, income and marital status) and psycho-social variables in step 2 (i.e. K6 score, self-rated mental health, self-rated physical health, LSNS-6 score, ATSPPHS-SF score, previous experience with mental health problems and previous experience with mental health treatment).
According to our first set of hypotheses examining the predictors of preferred amount of information, we expected that the previously outlined socio-demographic and psycho-social independent variables would be related to amount of information on medication treatment, counselling or psychological treatment, combination treatment and self-help treatment. A PCA of the four questions concerning preferred amount of information resulted in a one-factor solution. As a result, we computed one composite dependent variable, consisting of the four questions concerning preferred amount of information in the areas identified above, which served as the dependent variable in the hierarchical linear regression analysis.
In our second set of hypotheses related to older adults’ preferred content of information, we hypothesised that the previously outlined socio-demographic and psycho-social independent variables would be related to information content. In light of a three-factor solution that resulted from a PCA of 17 content of information variables, we computed three composite dependent variables: pharmacotherapy content (i.e. side-effects of medication treatment, possible addiction to medication, interaction effects of medication, medication management, length of time medications need to produce results and training of treatment provider); psychotherapy content (i.e. where psychological treatment will take place, what you do during psychological treatment, amount of psychological treatment required, length of treatment sessions, side-effects of psychological treatment and combination treatment); and content regarding treatment options and decision-making (i.e. when to seek treatment, how to recognise symptoms, treatment options, advantages and disadvantages of treatment options, and medication treatment options).
In our third set of hypotheses concerning older adults’ preferred formats of information, we included the same socio-demographic and psycho-social independent variables used to test previous hypotheses. A PCA of the four format variables (i.e. written form, heath-care provider, DVD and internet website) resulted in a four-factor solution. As such, we did not use the PCA, and dependent variables remained consistent with variables in the questionnaire.
Finally, according to our fourth set of hypotheses related to older adults’ preferred sources of information, we hypothesised that the previously outlined socio-demographic and psycho-social independent variables would be related to all information source variables. Results of a PCA on the ten source variables failed to reveal a statistically and theoretically clear factor solution. We therefore created three composite dependent variables based on theoretical and applied knowledge: independent learning (i.e. community newspaper, self-help book and internet); heath-care professionals (i.e. primary care physician, mental health professional and pharmacist); and family and friends (i.e. spouse or romantic partner, child/children, close friend(s) and sibling(s)).
Results
Sample description
Table 1 shows the demographic, health-related and psycho-social characteristics of the N = 229 older adults who completed the mental health information questionnaire. Results of independent samples t-tests indicated that medical clinic and senior centres samples differed significantly on the following demographic characteristics: age, education, household income and racial background. The two samples did not differ significantly on other variables. Given that these socio-demographic characteristics were not strong or consistent significant predictors of information preferences in subsequent regression analyses, analyses focused on the total sample of older adults. Analysing results with the total sample of older adults provided adequate statistical power for analyses. Respondents scored within the normative range for social connectedness on the LSNS-6 and within the normal range for distress on the K6, and mean scores on the ATSPPHS-SF indicated relatively favourable attitudes towards seeking mental health treatment.
Table 1. Older adult sample characteristics

Notes: 1. 1 = poor, 2 = fair, 3 = good, 4 = very good, 5 = excellent. SD: standard deviation. LSNS-6: six-item Lubben Social Network Scale. K6: six-item Kessler Psychological Distress scale. ATSPPHS-SF: Attitudes Toward Seeking Professional Psychological Help Scale – Short Form.
Highest level of education = Total number of years of educational attainment.
Older adults’ mental health information preferences
When rating their level of familiarly with the types of help for mental health problems (e.g. stress, anxiety and depression), the majority of respondents (57.2%) reported being unfamiliar, compared to 19.2 per cent who reported being moderately familiar and 21.4 per cent who reported being very familiar with the types of help for mental health problems.
Amount
As shown in Table 2, nearly two-thirds of respondents preferred detailed information on psychological, pharmacological and combined treatment options; whereas roughly half of respondents preferred detailed information on self-help approaches. These differences were not statistically significant based on overlapping confidence intervals.
Table 2. Older adults’ preferences regarding amount of information
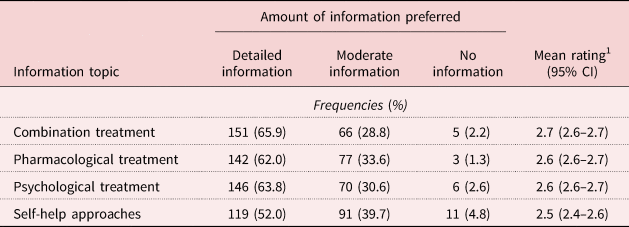
Notes: N = 229. 1. 1 = no information preferred, 2 = moderate information preferred (brief pamphlet or one-page fact sheet), 3 = detailed information preferred (two to six pages). CI: confidence interval.
Content
Table 3 shows that, overall, a large proportion of older adults rated a wide variety of mental health information content items as very important. When examining the three composite scores, namely the pharmacotherapy factor, treatment options and decision-making factor, and psychotherapy factor, it is evident that the confidence intervals for psychotherapy and treatment options and decision-making do not overlap with the pharmacotherapy confidence interval, suggesting that, overall, the pharmacotherapy content area may be more preferred by older adult respondents. When responding to the question concerning other information that they would like to know prior to making a decision about finding help for a mental health problem, participants identified the following content areas: how to recognise the seriousness of a mental health problem (distinguishing mild, moderate and severe symptoms); first steps to take in seeking treatment; confidentiality of treatment; length of waiting time to meet with a treatment provider; number of psychological treatment sessions that might be covered through insurance plans; and information on alternative treatment options.
Table 3. Older adults’ preferences regarding content of information

Notes: N = 229. 1. 1 = not important, 2 = moderately important, 3 = very important. CI: confidence interval.
Format
Table 4 depicts that over half (59.9%) of respondents rated information obtained through a discussion with their heath-care provider as very preferred, and this same proportion of participants (59.9%) rated information in written format as very preferred. One-third of participants (32.3%) rated information in DVD format as very important; and 27.1 per cent of participants rated information on the internet as very preferred. Older adults’ preference for discussion with a heath-care provider and written information, over DVDs and the internet, was significant, as indicated by non-overlapping confidence intervals. Participants identified the following as other information formats that they would find helpful if experiencing a mental health problem and looking for help: information received via telephone hotline/triage system, information received by text-messaging and email, and information received through home visits.
Table 4. Older adults’ preferences regarding format of information

Notes: N = 229. 1. 1 = not preferred, 2 = moderately preferred, 3 = very preferred. CI: confidence interval.
Source
As shown in Table 5, respondents indicated that they would be very likely to contact a variety of sources for mental health information. Over three-quarters of respondents reported that they would be very likely to contact their family doctor as a source of mental health information. Over half of respondents reported that they would be very likely to contact their spouse/romantic partner, or a mental health professional. Slightly less than half of respondents reported that they would be very likely to contact their child/children as a source of mental health information. Independent learning sources, including a community newspaper, a recommended self-help book and the internet, were less favourably rated by respondents. Older adults’ preference to consult family and friends and health-care professionals, over independent learning sources, was significant, as indicated by non-overlapping confidence intervals. Further, older adults significantly preferred their family doctor as a source of mental health information, in comparison to all other source variables, with the exception of mental health professionals. Participants identified support groups, Health Links telephone hotline, community organisations and religious/spiritual advisors as other sources to consult if they were experiencing a mental health problem and were looking for help.
Table 5. Older adults’ preferences regarding source of information

Notes: N = 229. 1. 1 = not likely, 2 = moderately likely, 3 = very likely. CI: confidence interval.
Predictors of mental health information preferences
Amount
Together, socio-demographic and psycho-social variables accounted for 14 per cent of the variance in participants’ preference for amount of information, F(13,148) = 1.86, p < 0.05. Social isolation/support was a unique significant predictor of amount of information, with older adults who reported lower self-rated social isolation, and conversely, greater social support/connection, demonstrating a greater preference for a larger amount of information concerning mental health treatment.
Content
Three regression analyses predicted older adults’ preference for pharmacotherapy, psychotherapy, and treatment option and decision-making content of mental health information (see Table 6). For the preference for information on pharmacotherapy analysis, socio-demographic variables accounted for 12 per cent of the variance in step 1, F(6,160) = 3.74, p < 0.01. A greater preference to seek out pharmacotherapy-related information was associated with higher educational attainment and being married or in a common-law relationship.
Table 6. Regressions of socio-demographic and psycho-social characteristics on content of information

Notes: N = 229. 1. 0 = female, 1 = male. 2. 0 = White, 1 = non-White. 3. 0 = Can $0–34,999, 1 = 35,000–60,000+. 4. 0 = single/previously married, 1 = married/common law. SE: standard error. K6: six-item Kessler Psychological Distress scale. LSNS-6: six-item Lubben Social Network Scale. ATSPPHS-SF: Attitudes Toward Seeking Professional Psychological Help Scale – Short Form.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
The socio-demographic predictors were no longer significant when the psycho-social variables were added in step 2, which accounted for an additional 17 per cent of the variance, F(7,153) = 5.05, p < 0.001. Participants who reported lower self-rated social isolation (greater social support), more favourable attitudes towards seeking professional psychological help, and previous experience with stress, anxiety or depression, demonstrated a greater preference to receive information focused on pharmacotherapy. The experience of greater psychological distress was associated with a decreased preference to receive information concerning pharmacological treatment. Together, socio-demographic and psycho-social variables accounted for 29 per cent of the variance in participants’ preferences for pharmacotherapy content of information, F(13,153) = 4.75, p < 0.001.
A second regression analysis examined socio-demographic and psycho-social characteristics associated with participants’ preference for information on psychotherapy. Neither socio-demographic variables entered in step 1 of this analysis nor psycho-social variables entered in step 2 of this analysis significantly predicted participants’ preference for information on psychotherapy.
A third regression analysis examined predictors of participants’ preference for information on mental health treatment options and decision-making. The socio-demographic variables in step 1 of the model did not predict participants’ information preferences, whereas the psycho-social variables in step 2 accounted for an additional 21 per cent of the variance in participants’ preference for information on treatment options and decision-making, F(7,153) = 6.11, p < 0.001. Participants who reported more favourable attitudes towards seeking professional psychological help and previous experience with stress, anxiety and depression, demonstrated a greater preference for information related to treatment options and decision-making. Together, socio-demographic and psycho-social variables accounted for 27 per cent of the variance in participants’ preference for this type of content of information, F(13,153) = 4.26, p < 0.001.
Format
As shown in Table 7, four regression analyses examined socio-demographic and psycho-social characteristics associated with older adults’ preferred formats of mental health-related information (i.e. information presented via written format, discussion with a heath-care provider, in DVD format and on the internet). The first two regression models examining socio-demographic and psycho-social variables associated with information presented in written format and through discussion with a heath-care provider were non-significant.
Table 7. Regressions of socio-demographic and psycho-social characteristics on format of information

Notes: N = 229. 1. 0 = female, 1 = male. 2. 0 = White, 1 = non-White. 3. 0 = Can $0–34,999, 1 = 35,000–60,000+. 4. 0 = single/previously married, 1 = married/common law. SE: standard error. K6: six-item Kessler Psychological Distress scale. LSNS-6: six-item Lubben Social Network Scale. ATSPPHS-SF: Attitudes Toward Seeking Professional Psychological Help Scale – Short Form.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
The third regression analysis examined socio-demographic and psycho-social variables associated with participants’ preference for information presented in DVD format. Socio-demographic variables accounted for 9 per cent of the variance in step 1 of this analysis, F(6,156) = 2.63, p < 0.05. Older age was a significant demographic predictor of preference of information presented in DVD format. Together, socio-demographic and psycho-social variables accounted for 16 per cent of the variance in participants’ preference to receive information in DVD format, F(13,149) = 2.13, p < 0.05. Age remained a significant predictor of information format preference in step 2, and psychological distress emerged as a significant unique psycho-social predictor of preference for mental health information in DVD format, whereby greater distress was associated with a decreased preference for this format of information.
The fourth regression analysis examined socio-demographic and psycho-social characteristics associated with participants’ preference for information presented on the internet. Socio-demographic characteristics accounted for 15 per cent of the variance in step 1 of this analysis, F(6,156) = 4.56, p < 0.001. Together, socio-demographic and psycho-social variables accounted for 19 per cent of the variance in participants’ preference to receive information on the internet, F(13,149) = 2.74, p < 0.01. Educational attainment remained a significant predictor of preference of Web-based information in step 2 of the analysis.
Source
Three regression analyses examined socio-demographic and psycho-social characteristics associated with older adults’ preference for source of mental health information (i.e. family and friends, heath-care professionals and independent learning) (see Table 8). In the first regression analysis examining variables associated with preference to seek information from family and friends, socio-demographic variables accounted for 9 per cent of the variance, F(6,156) = 2.48, p < 0.05. Sex emerged as a unique significant predictor, with men being less likely to seek information from this source. Psycho-social variables added in step 2 of the model accounted for an additional 13 per cent of the variance, F(7,149) = 3.66, p < 0.01. Together, socio-demographic and psycho-social variables accounted for 22 per cent of the variance in participants’ preference to receive information from family and friends, F(13,149) = 3.25, p < 0.001. Sex remained a unique significant predictor in step 2, and lower self-reported social isolation (greater social support) emerged as an additional significant predictor of participants’ preference to receive information from family and friends.
Table 8. Regressions of socio-demographic and psycho-social characteristics on source of information

Notes: N = 229. 1. 0 = female, 1 = male. 2. 0 = White, 1 = non-White. 3. 0 = Can $0–34,999, 1 = 35,000–60,000+. 4. 0 = single/previously married, 1 = married/common law. SE: standard error. K6: six-item Kessler Psychological Distress scale. LSNS-6: six-item Lubben Social Network Scale. ATSPPHS-SF: Attitudes Toward Seeking Professional Psychological Help Scale – Short Form.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
The second regression analysis predicted participants’ preference to consult heath-care professionals as a source of mental health information. Although socio-demographic variables entered in step 1 were not significant predictors, psycho-social variables added in step 2 accounted for an additional 21 per cent of the variance in participants’ preference to consult these sources, F(7,148) = 6.01, p < 0.001. Older age, lower self-rated physical health, lower self-reported social isolation (greater social support) and more favourable attitudes towards seeking professional psychological help were associated with a greater likelihood of consulting this source of information. Together, socio-demographic and psycho-social variables accounted for 27 per cent of the variance in participants’ preference to consult this source of information, F(13,148) = 4.12, p < 0.001.
The third regression analysis predicted participants’ preference to consult independent learning sources for mental health information. Neither socio-demographic nor psycho-social variables significantly predicted participants’ preference for this informational source.
Discussion
We aimed to examine the mental health information preferences of community-dwelling older adults, as well as the socio-demographic and psycho-social predictors of mental health information preferences. Our findings contribute to an underdeveloped and increasingly important line of research in the area of geriatric mental health and underlie the importance of older adults’ preference for shared decision-making in health care. Furthermore, our findings should be considered from the perspective of social theories of help-seeking such as the network episode model which emphasises that pathways to mental health treatment are dynamic and influenced by individual, social and treatment system factors (Pescosolido et al., Reference Pescosolido, Boyer, Medina, Aneshensel, Phelan and Bierman2013). This model has been shown to capture the experiences of older adults with mental health problems who are especially likely to ‘muddle through’ the help-seeking process (Berard et al., Reference Berard, Mackenzie, Reynolds, Thompson, Koven and Beatie2020; Reynolds et al., Reference Reynolds, Medved, Mackenzie, Funk and Koven2020; Beatie et al., Reference Beatie, Mackenzie, Thompson, Koven, Eschenwecker and Walkerin press).
When asked to rate their level of familiarity with the types of help available for mental health problems, a slight majority of participants (57.2%) reported being unfamiliar with treatment options. This finding is consistent with the mental health literacy literature suggesting that many older adults have limited knowledge concerning the recognition, management and prevention of mental health problems (Fisher and Goldney, Reference Fisher and Goldney2003; Farrer et al., Reference Farrer, Leach, Griffiths, Christensen and Jorm2008; Wetherell et al., Reference Wetherell, Petkus, McChesney, Stein, Judd, Rockwell, Sewell and Patterson2009; Hadjimina and Furnham, Reference Hadjimina and Furnham2017). This finding furthermore provides evidence to support targeted strategies by service providers, policy makers and others to improve older adults’ knowledge concerning treatment options for mental health problems.
Content
The low level of familiarity with treatment options did not appear to detract from older adults’ desire to obtain information on a wide variety of topics related to mental health problems and treatment. Older adults rated a variety of mental health information content items in the areas of pharmacotherapy, psychotherapy, and treatment options and decision-making as very important. These highly rated content items suggest that most older adults are interested in learning about various options when making mental health treatment decisions, suggesting a desire for balanced, evidence-based information in multiple treatment domains.
Participants rated information on pharmacotherapy as more important relative to information about treatment options and decision-making or information about psychotherapy. It is possible this finding reflects older adults’ overall experiences accessing heath-care services. This could also reflect appropriate concern about associated risks of treatment. This possibility is supported by the content items highly rated by respondents, including side-effects, interaction effects and possible addiction to medication. Research shows that older adults who seek treatment for mental health problems are most likely to access services from a primary care physician and, correspondingly, are more likely to pursue pharmacotherapy than other treatment options (Bogner et al., Reference Bogner, De Vries, Maulik and Unützer2009; Nyunt et al., Reference Nyunt, Chiam, Kua and Ng2009; Préville et al., Reference Préville, Vasiliadis, Boyer, Goldfarb, Demers, Brassard and Béland2009; Cairney et al., Reference Cairney, Corna and Streiner2010; Han et al., Reference Han, Gfroerer, Colpe, Barker and Colliver2011; Lippens and Mackenzie, Reference Lippens and Mackenzie2011). Such findings are concerning as they may contradict older adults’ preferences; with some research demonstrating that older adults prefer psychological treatment in comparison to pharmacological treatment (e.g. Lundervold and Lewin, Reference Lundervold and Lewin1990; Rokke and Scogin, Reference Rokke and Scogin1995; Landreville et al., Reference Landreville, Landry, Baillargeon, Guérette and Matteau2001; Areán et al., Reference Areán, Alvidrez, Barrera, Robinson and Hicks2002; Wetherell et al., Reference Wetherell, Kaplan, Kallenberg, Dresselhaus, Sieber and Lang2004). Further to this, a recent qualitative study on the experiences of psychotropic medication use and decision-making for adults with intellectual disability highlighted that care-givers of older adults expressed a desire for involvement in shared decision-making concerning psychotropic medication. However, care-givers described that they were uninformed about key facts concerning medication, insufficiently included in decisions and lacked influence in decision-making (Sheehan et al., Reference Sheehan, Hassiotis, Strydom and Morant2019).
Amount
In addition to reporting a desire for a wide variety of informational topics related to mental health problems and treatments, nearly two-thirds of respondents preferred detailed information on psychological, pharmacological and combined treatment options, and half of respondents preferred detailed information on self-help approaches. This desire for detailed information may be problematic in practice. First, older adults may not easily have access to information that is as detailed as they want. Second, those currently experiencing a mental health problem and searching for treatment options may benefit more from concise information that enables more rapid decision-making. Future research should determine the amounts of information older adults prefer when they are actually in the process of seeking treatment for a current mental health problem. Future research is also needed to examine the effectiveness of self-help treatments, highlighted as a preference by older adults in our study.
Format
Findings examining preferred information formats indicated that overall, older adults prefer to obtain information through discussion with heath-care providers as well as information in written format, in comparison to information in DVD format and Web-based information. The current generation of older adults’ low-rated preference for Web-based information may pose an access barrier, given the current trend towards online health information exchange combined with decreased availability of paper-based information (Selwyn et al., Reference Selwyn, Gorard, Furlong and Madden2003). Older adults also have more difficulty locating and understanding online health information, relative to younger age groups (Agree et al., Reference Agree, King, Castro, Wiley and Borzekowski2015). Our finding emphasises that older adults should be provided with mental health information in a variety of formats and through a variety of sources, and supports prior research demonstrating that information should be available in both old (e.g. books, pamphlets) and new (e.g. internet) media formats to maximise uptake (Cunningham et al., Reference Cunningham, Walker, Eastwood, Westra, Rimas, Chen, Marcus, Swinson and Bracken2013). Although the sample of older adults in our study rated the internet as their least preferred source of information, given current statistics concerning internet use for health-related information worldwide, it is reasonable to expect that future cohorts of older adults will increasingly look to online options for health-related information (e.g. Dumitru et al., Reference Dumitru, Bürkle, Potapov, Lausen, Wiese and Prokosch2007; Atkinson et al., Reference Atkinson, Saperstein and Pleis2009; Fox and Duggan, Reference Fox and Duggan2013; Bujnowska-Fedak, Reference Bujnowska-Fedak2015). This finding also highlights the importance of systemic change in supporting older adults in their access and engagement with technology, with research describing that information and communication technologies are integral in older adults’ participation in society now and into the future (Selwyn et al., Reference Selwyn, Gorard, Furlong and Madden2003). Older adults’ preference to obtain information in discussion with a heath-care provider is also important to highlight, particularly in relation to their desire for detailed information, as this may be challenging in the context of the multiple demands and scheduling constraints faced by heath-care providers. This concern was highlighted in recent qualitative research (MacRae et al., Reference MacRae2018).
Source
Findings examining preferred information sources indicate that older adults may be most likely to contact their family, friends, family doctors and mental health professionals if they were to experience a mental health problem. These informational sources were more preferred in comparison to pharmacists and independent learning sources (i.e. community newspaper, self-help book and internet website). In line with findings in the area of preferred information formats, older adults desired external sources of information over self-directed sources. Although family and friends were a highly preferred source of information, these individuals may have limited knowledge about mental health treatment options, either prolonging the search for information and treatment or resulting in misinformation. This finding highlights the importance of creating balanced and evidence-based information on mental health problems and treatment options for older adults, to empower both those experiencing mental health problems and their close others in making important treatment-related decisions.
Given that older adults reported health-care professionals as another highly rated source of mental health information, it is important to consider how effective knowledge exchange could be expedited within health-care systems. Primary care physicians, as the most commonly visited health professional among older adults, do not often have sufficient time in a typical appointment to discuss treatment options and characteristics associated with options with older patients, who may also be experiencing a range of physical health problems (Scott et al., Reference Scott, MacKenzie, Chipperfield and Sareen2010; El-Gabalawy et al., Reference El-Gabalawy, Mackenzie and Sareen2016). The Canadian Medical Association general practitioner guideline of 10–15 minutes for a routine patient appointment makes it particularly difficult for older adults with complex, comorbid health problems to have their information and health-related needs met (Canadian Medical Association, 2012; El-Gabalawy et al., Reference El-Gabalawy, Mackenzie and Sareen2016). As a result, geriatric depression and anxiety can be undetected, undiagnosed and undertreated in primary care settings, leaving many older adults without appropriate help (Unützer, Reference Unützer2002; Park and Unützer, Reference Park and Unützer2011). Further, although older adults rated mental health professionals as a highly preferred source of mental health information, there is a scarcity of specialty mental health resources in Canada and other countries, and of evidence-based integrated service delivery, such as collaborative care/shared care models combining primary care with specialty mental health care, despite the benefits and opportunities (Speer and Schneider, Reference Speer and Schneider2003; Bartels et al., Reference Bartels, Coakley, Zubritsky, Ware, Miles, Arean, Chen, Oslin, Llorente, Costantino, Quijano, McIntyre, Linkins, Oxman, Maxwell and Levkoff2004; Patel et al., Reference Patel, Belkin, Chockalingam, Cooper, Saxena and Unützer2013).
Predictors of mental health information preferences
Confirming our hypotheses, findings indicated that overall, socio-demographic and psycho-social characteristics accounted for some of the variance in predicting older adults’ preferences for amount, content, format and source of mental health information. The independent variables that had the strongest, most consistent effects across dependent variables were attitudes towards seeking professional psychological help, social connectedness, previous mental health problems and current distress. It is important to interpret these findings with caution, considering the small sample size and low beta coefficients in the current research.
Attitudes are important predictors of treatment-seeking preferences (Cramer, Reference Cramer1999; Mackenzie et al., Reference Mackenzie, Gekoski and Knox2006, Reference Mackenzie, Scott, Mather and Sareen2008; ten Have et al., Reference ten Have, de Graaf, Ormel, Vilagut, Kovess and Alonso2010). Our study found that more favourable attitudes towards treatment-seeking were associated with a greater preference for information concerning pharmacological treatment options and information related to treatment options and decision-making. Favourable attitudes towards treatment-seeking also predicted a greater preference for seeking mental health treatment-related information from heath-care professionals.
A strong, consistent finding in our study was that increased social support/connectedness predicted a preference for receiving more information, as well as an increased likelihood of consulting heath-care professionals and family and friends as sources for mental health information. This supports research by Askelson et al. (Reference Askelson, Campo and Carter2011) within the area of information preferences for cancer treatments. This finding is also consistent with literature in the area of ageing and help-seeking, suggesting that increased social support and increased informational support are associated with more positive attitudes towards seeking mental health services (e.g. Park et al., Reference Park, Jang, Lee, Schonfeld and Molinari2012; Guruge et al., Reference Guruge, Thomson, George and Chaze2015; Kessler et al., Reference Kessler, Agines and Bowen2015). In contrast, more socially isolated older adults without close others (with whom to discuss information and treatment options) may prefer briefer information.
Contrary to our hypothesis, greater distress predicted lower preference for information on pharmacotherapy. Since emotional distress often leads to decrements in attention, short-term memory and information processing (e.g. Ellenbogen et al., Reference Ellenbogen, Schwartzman, Stewart and Walker2002, Reference Ellenbogen, Carson and Pishva2010; Vitaliano et al., Reference Vitaliano, Zhang and Scanlan2003, Reference Vitaliano, Echeverria, Yi, Phillips, Young and Siegler2005), one explanation for this finding is that mental health information is more likely to be understood, processed and recalled when distress is mild. The information may be more digestible, and thus useful, when distress is still mild, such as at earlier stages of a mental health problem.
We found that previous mental health treatment did not emerge as a significant predictor of information preferences, which may reflect the effectiveness/ineffectiveness of participants’ past treatment experiences. It is possible that participants who experienced ineffective treatment may have rated a preference for more detailed information, and those who experienced effective treatments less, thereby cancelling out any effect.
Although psycho-social characteristics demonstrated the strongest, most consistent effects across dependent variables, several noteworthy findings emerged regarding age, education and sex. First, although our sample ranged in age from 50 to 100 years, age only emerged as a unique significant predictor of information in DVD format, with older age being associated with increased preference for this format of information. Similarly, education emerged as a unique significant predictor of preference for Web-based format of information, with higher educational attainment associated with a greater preference for this format of information. In line with the aforementioned trend towards increased use of the internet for health-related information over time, it will be important for future investigations to examine ways to decrease the potential barrier of educational attainment to increase accessibility of information. Lastly, in support of previous findings in the area of treatment-seeking for mental health problems (e.g. Byers et al., Reference Byers, Arean and Yaffe2012; Mackenzie et al., Reference Mackenzie, Reynolds, Cairney, Streiner and Sareen2012), sex emerged as a unique predictor of information source in our study; males did not prefer to seek information from family and friends, relative to females.
Limitations and future directions
Overall, the demographic and health-related characteristics in the present sample are similar to those of older adults from Statistics Canada datasets (Statistics Canada, 2006, 2015). Future research, however, would benefit from obtaining increased heterogeneity in sampling, to recruit persons from a variety of racial and ethnic groups, recent immigrants, and persons with lower levels of educational attainment and income, and findings of this study may not be generalisable to global populations of older adults.
Socio-demographic and psycho-social characteristics accounted for 16–29 per cent of the variance in older adults’ preferences for amount, content, format and source of mental health information in our study. This suggests that additional variables are contributing to a large portion of the variance unexplained by the variables included in the current study and paves the way for future investigation related to older adults’ mental health information preferences.
The nature and design of this research was appropriate given the absence of research in this particular area. Although information about participants’ history of physical and mental health problems was gathered by self-report, prior research has found adequate to good reliability between self-reported physical health problems and those diagnosed by health professionals (Kriegsman et al., Reference Kriegsman, Penninx, van Eijk, Boeke and Deeg1996). Nevertheless, the correlational, cross-sectional design of the current research imposes a limitation in the interpretation of findings regarding predictors of mental health information preferences. Future research using experimental methods to examine predictors of mental health information preferences over time, and following mental health literacy interventions in particular, are necessary.
Finally, we recommend future research also explores actual physical and mental health-related decision-making practices of older adults, paying particular attention to decisions about the amount, content, format and source of information. Situating this research within a broad social model of help-seeking which also considers social aspects of decision-making would be especially helpful.
Experimental research comparing preference for, and perceived helpfulness of, health-related information, as well as research examining the behavioural outcomes of health-related information (e.g. utilisation, mental health help-seeking) among older adults may be beneficial, as this area of patient-oriented research continues to grow.
Conclusion
It is important for researchers, heath-care professionals and policy makers in the areas of ageing, mental health and social gerontology to enable and improve the mental health literacy of older adults, further empowering them to participate in shared decision-making in mental health help-seeking. By elucidating the information preferences of older adults, our study represents an important step in this growing area of research and practice, and has special implications for collaborative care/shared care models that integrate primary care services and specialty mental health services. Equipping older adults with information pertaining to mental health treatment options, in the amounts, formats and from sources they prefer, will help improve mental health help-seeking and specific decisions concerning treatments, clarify pathways to service use, and ultimately lead to better mental and physical health outcomes. By coming together as a community of practice within the ageing, mental health and social gerontology fields, prioritising research and practice initiatives focusing on the empowerment of older adults in mental health help-seeking, we can make further strides to combat pervasive systemic patterns of ageism and system-induced passivity.
Acknowledgements
The authors would like to acknowledge the contributions of the late Dr John Walker, Professor Emeritus, Department of Clinical Health Psychology, University of Manitoba. Dr Walker provided integral support and mentorship throughout this project and is dearly missed. We extend thanks to Dr Laura Funk for her research consultation and to the participants who were involved in this research. We also acknowledge funding from the Canadian Institutes of Health Research and the University of Manitoba Centre on Aging which allowed us to complete this work.
Financial support
This work was supported by the Canadian Institutes of Health Research (KR, Canada Graduate Scholarship Doctoral Research Award); and the University of Manitoba Centre on Aging (KR).
Ethical standards
The study received Institutional Review Ethics Board approval.








