Introduction
Persons who are homeless experience a high burden of comorbid physical and mental health conditions that intersects with ongoing social and economic disadvantages (Luchenski et al., Reference Luchenski, Maguire, Aldridge, Hayward, Story, Perri and Hewett2018). Even in high-income nations with availability of universal health insurance, the co-occurrence of psychiatric illness, substance use, infectious diseases, and traumatic brain injury is remarkably common in this population and is associated with premature mortality (Aldridge et al., Reference Aldridge, Story, Hwang, Nordentoft, Luchenski, Hartwell and Hayward2018; Fazel, Geddes, & Kushel, Reference Fazel, Geddes and Kushel2014). Cross-sectional studies suggest that a greater number of co-occurring illnesses is also associated with poorer role functioning in homeless youth and adults (Barbic et al., Reference Barbic, Jones, Woodward, Piercy, Mathias, Vila-Rodriguez and Honer2018; Vila-Rodriguez et al., Reference Vila-Rodriguez, Panenka, Lang, Thornton, Vertinsky, Wong and Honer2013) and with greater functional impairment in older adults (Brown, Kiely, Bharel, & Mitchell, Reference Brown, Kiely, Bharel and Mitchell2012). Quality of life (QoL) also tends to be lower among homeless persons and has been linked with higher rates of psychiatric and substance use disorders (Gentil, Grenier, Bamvita, Dorvil, & Fleury, Reference Gentil, Grenier, Bamvita, Dorvil and Fleury2019; Hubley, Russell, Palepu, & Hwang, Reference Hubley, Russell, Palepu and Hwang2014) and viral co-infection (Tsui, Bangsberg, Ragland, Hall, & Riley, Reference Tsui, Bangsberg, Ragland, Hall and Riley2007).
An underappreciated dimension of illness burden in homeless persons is the consequential cognitive dysfunction or impairment. While an estimated 25% of persons exhibit global impairment (Depp, Vella, Orff, & Twamley, Reference Depp, Vella, Orff and Twamley2015), upwards of 75% of homeless adults exhibit clinically relevant verbal memory impairment in addition to domain-specific difficulties in attention, processing speed, and executive functions (mental flexibility, cognitive control, risky decision making; Gicas et al., Reference Gicas, Giesbrecht, Panenka, Lang, Smith, Vila-Rodriguez and Thornton2017; Stergiopoulos et al., Reference Stergiopoulos, Cusi, Bekele, Skosireva, Latimer, Schütz and Rourke2015). A similar profile of cognitive impairments is also observed in homeless youth (Barone et al., Reference Barone, Yamamoto, Richardson, Zivanovic, Lin and Mathias2019; Fry, Langley, & Shelton, Reference Fry, Langley and Shelton2017; Waclawik et al., Reference Waclawik, Jones, Barbic, Gicas, O'Connor, Smith and Thornton2019). Among homeless older adults (≥ 50 years), the rate of cognitive impairment is estimated to be 3–4 times higher than what would be expected for adults aged 70 years and older within the general population (Hurstak et al., Reference Hurstak, Johnson, Tieu, Guzman, Ponath, Lee and Kushel2017). Moreover, emergent longitudinal evidence indicates accelerated cognitive decline (Gicas et al., Reference Gicas, Jones, Thornton, Petersson, Livingston, Waclawik and Honer2020) and persistent or worsening functional impairment (Brown et al., Reference Brown, Guzman, Kaplan, Ponath, Lee and Kushel2019), raising concern around issues of chronic disability and possible future dementia in this population.
In general, there is a clear relationship between neurocognition and functional outcomes in healthy and patient populations (Morgan & Heaton, Reference Morgan, Heaton, Grant and Adams2009). Memory and executive function are critical to managing medications and health appointments, seeking and maintaining gainful employment, and maintaining social relationships (Gorman, Foley, Ettenhofer, Hinkin, & van Gorp, Reference Gorman, Foley, Ettenhofer, Hinkin and van Gorp2009). In a large meta-analysis of persons with schizophrenia spectrum disorders, overall cognitive functioning predicted community functioning, including QoL, with an overall medium effect size, but with the strongest domain-specific effects for verbal learning and memory (vLM), and processing speed (Halverson et al., Reference Halverson, Orleans-Pobee, Merritt, Sheeran, Fett and Penn2019). Cognition is likely to play an especially important role in community functioning and QoL among homeless persons with significant physical and mental comorbid conditions given the harsh realities of their day-to-day living environment. Everyday activities are apt to be more challenging due to systemic barriers in accessing health care services (Argintaru et al., Reference Argintaru, Chambers, Gogosis, Farrell, Palepu, Klodawsky and Hwang2013), ongoing discrimination and stigma faced in relation to perceived cognitive (Backer & Howard, Reference Backer and Howard2007) and mental health status (Mejia-Lancheros et al., Reference Mejia-Lancheros, Lachaud, Woodhall-Melnik, O'Campo, Hwang and Stergiopoulos2021), and a general inability to modify one's environment to match level of need (Kushel, Reference Kushel2011).
To date, there are very few studies that have explicitly examined the cognitive determinants of functional outcomes in homeless persons. In a sample of homeless veterans newly enrolled in a supportive housing program, social cognitive ability, but not global cognitive ability, was associated with the level of community integration (role functioning, social connections; Horan et al., Reference Horan, Wynn, Gabrielian, Glynn, Hellemann, Kern and Green2019). In contrast, impairments in mental flexibility and global cognition were associated with poorer instrumental activities of daily living (taking medications, using public transportation, budgeting finances) in homeless older adults (Hurstak et al., Reference Hurstak, Johnson, Tieu, Guzman, Ponath, Lee and Kushel2017). Among homeless youth, better working memory performance was a predictor of progression to independent living (Fry, Langley, & Shelton, Reference Fry, Langley and Shelton2020). Further investigations delineating the cognitive contributions to specific functional outcomes will help highlight tangible rehabilitation targets, essential to the success of interventions and service delivery models for this vulnerable population who frequently suffer the double burden of homelessness and mental illness.
The primary aim of the current study is to examine the specific contributions of cognitive functioning to community functioning and subjective QoL within a large Canadian sample of homeless adults with mental illness enrolled in a randomized controlled trial of Housing First (HF) and followed for up to 6 years. Given the dynamic nature of risk factors associated with functional outcomes in homeless persons, this study adopts a more nuanced approach by examining individual cognitive and functional trajectories and their co-variation. A cross-sectional snapshot of these associations may not reveal the full picture because some mental and physical illnesses may naturally ebb and flow in terms of their presence and acuity and transiently dysregulate functioning. An important secondary aim of this study is to evaluate the potential protective effect of resilience on functional outcomes in the context of cognitive impairment. Resilience is broadly defined as the ability to cope with and adapt to adversity and has been found to be positively associated with community functioning in homeless veterans (Greenberg et al., Reference Greenberg, Wynn, Lee, Hellemann, Gabrielian and Green2019).
It is hypothesized that better domain-specific cognitive performance (verbal learning and memory [vLM], complex processing speed and cognitive flexibility [PSCF]) will be associated with better community functioning and QoL over time after accounting for the effects of age, early childhood adversity, psychiatric illness, chronic physical health conditions, and resilience. It is further anticipated that resilience may confer a modification effect, whereby higher levels of resilience may enable individuals to maintain better community functioning and QoL despite poorer cognitive functioning.
Materials and methods
This study used data collected at the Toronto site as part of the At Home/Chez Soi (AH/CS) study, a large Canadian multi-city randomized controlled trial of HF for homeless adults with mental illness (Goering et al., Reference Goering, Streiner, Adair, Aubry, Barker, Distasio and Zabkiewicz2011). To briefly summarize, individuals who were randomly assigned to receive HF were provided with a rent supplement for their preferred housing within the community, as well as supportive mental health services (intensive case management or assertive community treatment) tailored to their level of need (moderate or high). Individuals assigned to the control group received treatment as usual (TAU), which consisted of the usual supports that were available to them in their community, including housing and mental health support services.
Participants
Phase 1 of the original study enrolled 575 participants at the Toronto, Canada site between October 2009 and June 2011 and followed participants up to April 2013. In an extension of the original Toronto site study (Phase 2), 414 participants re-consented to further follow-up between July 2014 and March 2017. Eligibilities for inclusion in the AH/CS study were (i) being at least 18 years old, meeting criteria for a mental disorder (with or without a substance use disorder); (ii) not currently receiving services by an assertive community treatment or intensive case management program; (iii) and being absolutely homeless or precariously housed. Participants were recruited through local agencies and programs that frequently encounter homeless persons, including shelters, drop-in centres, inpatient programs, community mental health teams, and criminal justice programs. For the current study, participants were eligible for inclusion if they had at least one follow-up visit that involved completion of cognitive and functional outcome assessments.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All participants provided written informed consent. The Toronto arm of the AH/CS study was approved by St. Michael's Hospital research ethics board and the larger national multi-site study was registered with the International Standard Randomized Control Trial Number Register (42520374).
Cognitive measures
A brief cognitive battery was administered by trained research assistants to participants at 6 and 24 months after the initial interview date for AH/CS, Phase 1, and at 6 and 18 months following enrolment in AH/CS, Phase 2. vLM was assessed with the Hopkins Verbal Learning Test Revised (HVLT-R) using the total immediate recall and delayed recall scores (Benedict, Schretlen, Groninger, & Brandt, Reference Benedict, Schretlen, Groninger and Brandt1998). Psychomotor speed and attention were measured with the Digit Symbol Coding subtest of the Wechsler Adult Intelligence Scale Revised (total correct score; Wechsler, Reference Wechsler1981); and with the Trail Making Test Part A (total time to completion, truncated to 150 s; Reitan, Reference Reitan1958). Cognitive flexibility, a component of executive functioning, was measured with the Trail Making Test Part B as the total time to completion truncated to a maximum of 300 s (Reitan, Reference Reitan1958). Cognitive scores were considered invalid if examiner notes indicated the presence of any extraneous factors that may have substantially influenced performance, such as difficulty comprehending task instructions, language barriers, extreme fatigue, vision problems, and substance or alcohol intoxication. All cognitive scores across time points were converted to z-score units using the baseline mean and standard deviation of the sample. Total scores on each part of the Trail Making Test were multiplied by −1 so that lower scores represented poorer performance consistent with the other measures. Cognitive z-scores at each time point were averaged to create two factor scores in line with previously identified cognitive factors in the AH/CS data (Stergiopoulos et al., Reference Stergiopoulos, Naidu, Schuler, Bekele, Nisenbaum, Jbilou and Rourke2019). The vLM factor was composed of the HVLT-R immediate and delayed recall scores, and the PSCF factor was composed of the digit symbol total score, and Trail Making Test total scores from Part A and B.
Functional outcome measures
Proximal to each cognitive testing session, self-report scales assessing community functioning and QoL were administered (98.9% same day, 1.1% within 6 weeks). Community functioning was measured with the total score from the Multnomah Community Ability Scale (MCAS), a 17-item questionnaire that asks participants questions about their community behaviours and social interactions, coping skills, and adaptations (Barker, Barron, McFarland, & Bigelow, Reference Barker, Barron, McFarland and Bigelow1994). Higher MCAS scores reflect higher levels of community functioning. QoL was measured with the total score from Lehman's 20-item QoL interview that asks participants to rate how they feel about different aspects of their life, organized into six subscales (family, finance, leisure, living situation, safety, social) with an additional final item that assesses overall life satisfaction (Uttaro & Lehman, Reference Uttaro and Lehman1999). All items are measured on a 7-point scale, with a maximum possible score of 140, and higher scores indicating better QoL. The 20 items on this scale are considered to measure subjective QoL, which emphasizes an individual's self-evaluation and perception of their life and how their personal expectations and goals intersect with the broader social and cultural value systems they are situated in (Hubley et al., Reference Hubley, Russell, Palepu and Hwang2014).
Covariates/risk and protective factors
A comprehensive structured interview was carried out at study entry to collect personal demographic information including age, gender (man or woman), education, and lifetime history of homelessness categorized as < 3 years or ⩾ 3 years. At the time of the initial interview, mental health and substance use disorders were assessed using the Mini International Neuropsychiatric Interview (MINI) and included a current diagnosis of major depression, psychotic disorder (including mood disorders with psychotic features), alcohol abuse or dependence, and substance abuse or dependence (Sheehan et al., Reference Sheehan, Lecrubier, Sheehan, Amorim, Janavs, Weiller and Dunbar1998). Chronic medical comorbidity (CMC) was indexed by summing the presence of self-reported physical health conditions at the initial AH/CS study interview. Physical health conditions included heart disease, stroke, diabetes, asthma, chronic bronchitis/emphysema, ulcers (stomach or intestinal), inflammatory bowel disease, migraine, thyroid problems, arthritis, kidney/bladder problems, liver disease (except hepatitis), and anaemia. Resilience was measured with the Connor-Davidson Resilience Scale-2 (CD-RISC2), a 2-item scale that captures individual ability to cope with adversity (Vaishnavi, Connor, & Davidson, Reference Vaishnavi, Connor and Davidson2007). Childhood adversity was measured at the AH/CS Phase 1, 18-month follow-up using the total score from the adverse childhood experience (ACE) scale that assesses abuse (physical, sexual, emotional), neglect, and household dysfunction that occurred prior to the age of 18 years (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards and Marks1998). Initial randomization to either the HF or TAU arm of the parent study was included to control for the effects of an intervention.
Statistical analyses
Descriptive statistics for the overall sample are reported using means (standard deviations) and medians (interquartile range) for continuous variables, and counts (proportions) for categorical variables. Pearson and point biserial correlation coefficients estimated the linear relationships between cognitive variables, functional outcomes, and covariates. A sensitivity analysis was conducted to examine possible differences in demographic and clinical characteristics between participants who were included v. excluded, using t tests and Χ2 tests.
As a first step in the longitudinal analyses, separate linear mixed-effects models with random intercepts and slopes were used to describe the trajectories of change for each domain-specific cognitive factor (vLM, PSCF) and functional outcomes (MCAS, QoL) while adjusting for the effects of demographic variables (age, gender, education) and treatment arm (HF v. TAU), entered as fixed effects. Time was calculated as years since the date of initial randomization and re-scaled so that time = 0 at the AH/CS, Phase-1's 6-month follow-up in alignment with the time of the initial cognitive and functional outcome evaluations. The association of demographic covariates with change in cognitive or functional trajectories over time was tested by including the interaction of time × covariate, one covariate at a time.
To test the association between time-varying cognitive factors (vLM, PSCF) and functional outcomes, separate linear mixed-effects models were run for each combination of cognitive factor and outcome (four models in total), including covariates identified in the screening phase. The main effect of the time-varying cognitive factor, as well as the interaction of the cognitive factor and time, were included in the models. The main effect can be interpreted as the average difference, over time, in the functional outcomes, for one unit of change in the cognitive factor. The interaction examines whether the effect of cognitive factor scores on functional outcomes varies over time. The moderating effect of resilience was evaluated by including an interaction between the cognitive factor score and CD-RISC2 scores. This interaction examines whether the main effect of the cognitive factors on functional outcomes over time differs by level of resilience (Singer & Willett, Reference Singer and Willett2003; p.171). An a priori decision was made to include putative risk and protective factors as covariates in the final models. These factors were selected to reflect physical and mental health conditions and adverse experiences commonly observed in homeless populations (Fazel et al., Reference Fazel, Geddes and Kushel2014); lifetime duration of homelessness, MINI diagnoses, ACE scores, CMC total count, and CD-RISC2 scores were included as fixed effects. The Akaike information criterion (AIC) was used to compare goodness-of-fit between models with different time-varying cognitive factors. All models were examined for normality of residuals and for multivariate outliers using Cook's distance and leverage values. Missing data on the outcome variables were imputed using full information maximum likelihood. Only participants with complete case data on the covariates were included. All statistical tests were two-tailed and statistical significance was defined as p < 0.05. All analyses were performed in R (R Core Team, 2020) using the lme4 package for the linear mixed-effects models (Bates, Mächler, Bolker, & Walker, Reference Bates, Mächler, Bolker and Walker2015).
Results
Of 575 participants enrolled in the study, 10 participants identified as transgender and were removed from the sample as there were too few individuals to enable subgroup analyses. A total of 456 completed at least two functional outcome assessments and 349 of these participants also had at least two valid cognitive assessments. Compared to participants who were included (n = 349) in the current study, those who were excluded (n = 226) had on average fewer years of education, a lower frequency of having received the HF intervention, and a lower rate of substance abuse or dependence diagnosis. However, these differences are modest and therefore not considered to meaningfully impact results. The full details of the sensitivity analysis are reported in online Supplementary Table S1. There were modest proportions of missing data on the following covariates: education (2.6%), lifetime homelessness (1.7%), ACE total score (7.2%), CD-RISC2 total score (13.5%), and CMC total count (2.3%). On average, participants completed approximately three out of four evaluations (mean = 3.6; s.d. = 0.7) and were followed for a mean of 4.3 years (s.d. = 1.1). Slightly over half of these participants (56.7%, n = 198) received the HF intervention and the remaining 43.3% (n = 151) were in the TAU study arm. The full sample characteristics are described in Table 1. At the initial evaluation, the correlation between vLM and PSCF cognitive factor scores was r = 0.47, and between outcome scores (MCAS and QoL) was r = 0.20. Additional correlations between continuous covariates and cognitive measures are reported in online Supplementary Table S2. The final sample size varied by analysis and is reported separately below for each of the main analyses of interest.
Table 1. Sample characteristics of participants with at least two cognitive and functional outcome assessments (N = 349)

Note. ACE = adverse childhood experience; CD-RISC2 = Connor-Davidson resilience scale-2; CMC = chronic medical comorbidities; IQR = interquartile range.
Description of cognitive and functional trajectories
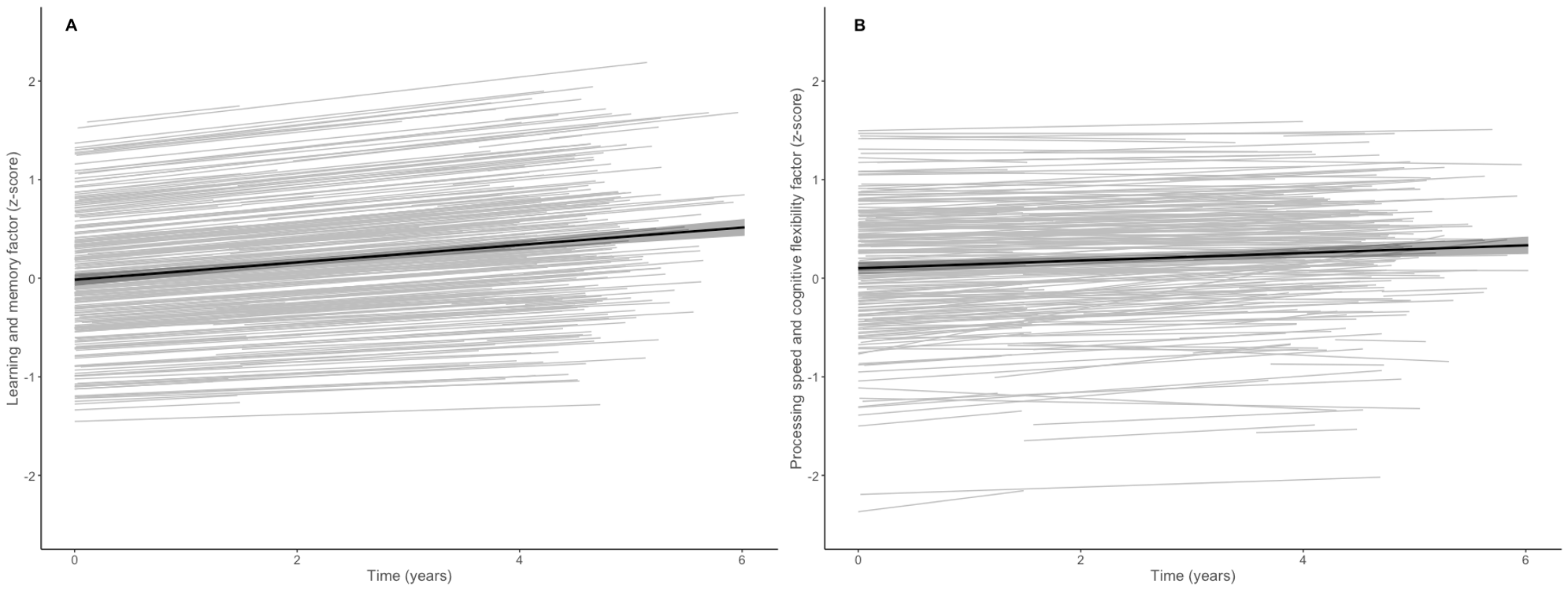
The results for each of the four descriptive trajectory models are summarized in online Supplementary Table S3. Briefly, in the first adjusted linear mixed-effects model, a linear increase in learning and memory performance was observed over time. Younger age, more years of education, and being a woman were associated with better learning and memory at initial cognitive evaluation, but were not associated with a change in cognitive functioning over time. The study intervention arm was unrelated to cognitive functioning. Similarly, processing speed and cognitive flexibility showed a linear increase with a significant age-by-time interaction indicating older individuals showed less improvement over time. Additionally, younger age and more years of education were associated with better processing speed and cognitive flexibility at initial evaluation, but gender and study intervention arm were not. The individual-level and average sample trajectories for cognitive measures are provided in online supplementary Fig. S1.
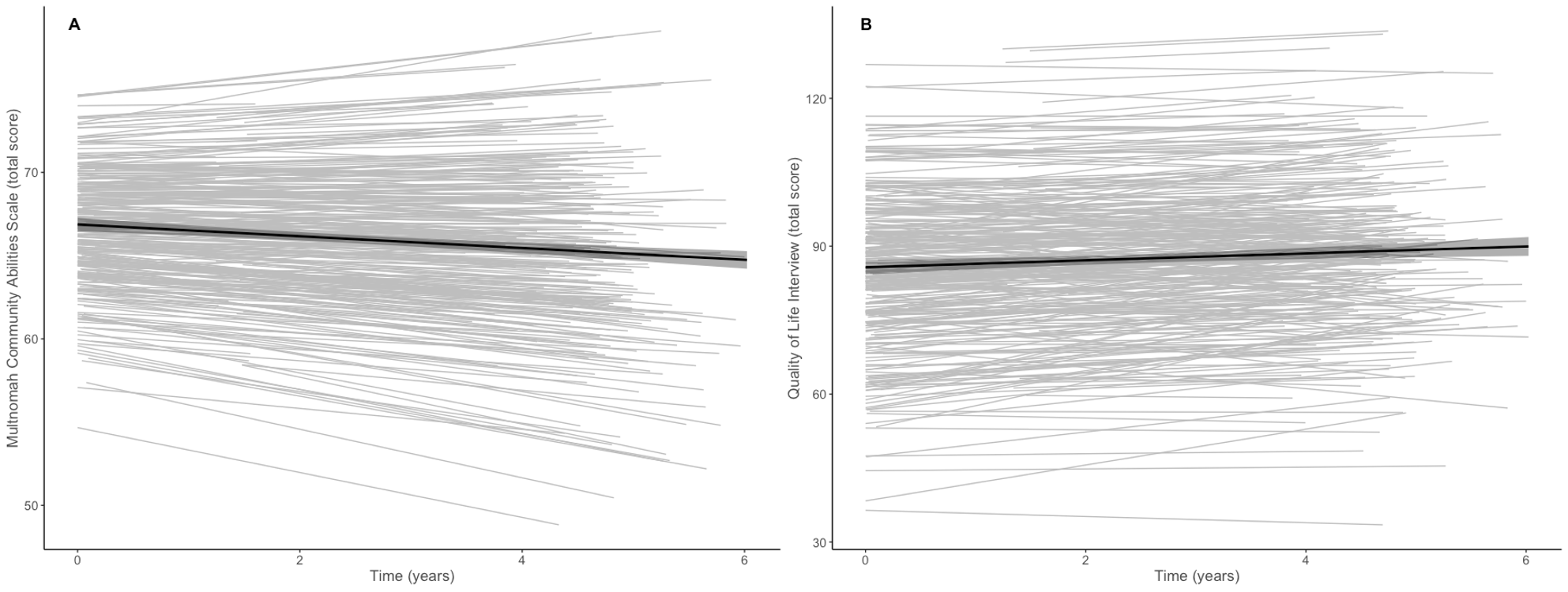
When MCAS total scores were examined as the outcome, a decline in community functioning was observed over time. More years of education, being a woman, and the HF intervention were associated with better community functioning at initial evaluation. In a separate adjusted model examining QoL scores, a significant linear increase in subjective QoL was observed over time. Receiving the HF intervention was associated with better QoL at baseline, but demographic variables were not. None of the covariates were related to change in either of the functional outcomes. Online Supplementary Fig. S2 provides the individual-level and average sample trajectories for each functional outcome.
Co-variation between cognition and functional outcomes over time
The results of the final adjusted models examining associations between time-varying cognitive factor scores and community functioning are summarized in Table 2. Briefly, a significant decline in community functioning was observed. Better learning and memory was associated with better community functioning, and this was consistent across time as evidenced by a non-significant cognition by time interaction. The non-significant interaction term was not included in the final model as reported in Table 2. Only education remained a significant covariate in the model showing a positive association with community functioning at initial evaluation. In a separate model, better processing speed and cognitive flexibility was also associated with better community functioning and remained consistent over time (i.e. no significant cognition by time interaction). Substance abuse/dependence was associated with worse community functioning at initial evaluation, but no other covariates were significant predictors in the final model. When comparing the two cognitive models, the overall fit as measured by the AIC was notably better when the processing speed and cognitive flexibility factor was included as the main predictor.
Table 2. Linear mixed-effects models examining the effects of cognition on community functioning over a 6-year period among homeless adults

Note. HF = housing first; CD-RISC2 = Connors-Davidson resilience scale; AIC = Akaike information criterion.
a Cognitive factor scores entered as time-varying predictors in each model.
The results of the final models examining QoL as the primary outcome are summarized in Table 3. There was a significant effect of time showing a linear increase in QoL over 6 years. However, neither vLM nor PSCF factor scores were associated with QoL. Further, cognition did not interact with time and therefore this term was not included in either model. Generally, receiving the HF intervention, less ACEs, and a greater level of resilience were independently associated with higher QoL at initial evaluation.
Table 3. Linear mixed-effects models examining the effects of cognition on subjective QoL over a 6-year period among homeless adults

Note. HF = housing first; CD-RISC2 = Connors-Davidson resilience Scale; AIC = Akaike information criterion.
a Cognitive factor scores entered as time-varying predictors in each model.
For each of the four main models, the level of individual resilience was examined as a moderator of cognitive-functional outcome associations. In contrast to our hypothesis, there were no significant interactions between cognitive factor scores and CD-RISC2 total scores in any of the models. Therefore, interaction terms were not retained in the final adjusted models.
Discussion
In a large Canadian sample of homeless adults with serious mental illness, differential associations between cognition measures and functional outcomes were observed. After adjusting for select risk and protective factors, composite indices of verbal learning and memory as well as processing speed and cognitive flexibility were positively associated with community functioning, but not with QoL, over a 6-year period. While greater individual resilience levels were independently associated with better QoL, resilience did not moderate the association between cognition and functional outcomes as expected. Altogether, cognition was the predominant predictor of community functioning, whereas select risk and protective factors (childhood adversity and resilience, respectively) were specifically associated with QoL, highlighting the need to consider the unique determinants of community functioning and QoL in the context of homelessness and mental illness.
In our study, additional descriptive analyses revealed improvements in cognitive functioning over time, likely attributable to practice effects (Wilson, Li, Bienias, & Bennett, Reference Wilson, Li, Bienias and Bennett2006), though older individuals showed less improvement in processing speed and cognitive flexibility, which may signal vulnerability to longer-term decline (Gicas et al., Reference Gicas, Jones, Thornton, Petersson, Livingston, Waclawik and Honer2020). We also observed that functional trajectories were characterized by a decline in community functioning and improvement in subjective QoL over the same 6-year period, a divergence possibly reflective of the ‘disability paradox’, which refers to the observation that people with significant and persistent disabilities tend to report experiencing good or excellent QoL (Albrecht & Devlieger, Reference Albrecht and Devlieger1999).
Our findings corroborate what is generally seen in stably housed psychiatric populations in that domain-specific cognitive functions are modestly but consistently associated with community functioning and QoL, though previous meta-analyses have combined these outcome domains (Fett et al., Reference Fett, Viechtbauer, Dominguez, Penn, van Os and Krabbendam2011; Halverson et al., Reference Halverson, Orleans-Pobee, Merritt, Sheeran, Fett and Penn2019) making it difficult to parse the unique cognitive contributions to each type of outcome. The current study is among the first to formally evaluate these differential associations among homeless adults. Our findings of positive associations between cognition and community functioning are similar to those of Schutt, Seidman, Caplan, Martsinkiv, and Goldfinger (Reference Schutt, Seidman, Caplan, Martsinkiv and Goldfinger2007), who reported that better cognitive functioning was associated with better community functioning at 18 months of follow-up among 112 homeless individuals with severe mental illness who were randomly assigned to independent housing or a group home. Their findings also indicated that the cognitive effects were dependent on the type of housing, highlighting how cognitive strengths may be leveraged to optimize functioning within particular social contexts and housing accommodations. Likewise, our findings are consistent with Stergiopoulos, Burra, Rourke, and Hwang (Reference Stergiopoulos, Burra, Rourke and Hwang2011) who reported that better performance on measures of verbal memory, processing speed, and executive functioning predicted functional capacity in a sample of psychiatric inpatients with schizophrenia that included 30 homeless persons and 21 demographic-matched housed controls. The authors found that cognitive flexibility was a particularly strong predictor of functional capacity relative to verbal memory; a pattern that was also observed in the current study. More recently, Mahmood et al. (Reference Mahmood, Vella, Maye, Keller, Van Patten, Clark and Twamley2021) reported strong associations between domain-specific and global cognition and functional capacity in a sample of 100 homeless adults. In contrast, a report by Horan et al. (Reference Horan, Wynn, Gabrielian, Glynn, Hellemann, Kern and Green2019) found no association between a global composite measure of cognition and community integration measured with the Role Functioning Scale in a sample of 176 homeless veterans. Heterogeneity in sample compositions and outcome measures are possible explanations for these discrepant findings.
In our study, there was no association between cognition and subjective QoL as initially expected. QoL is a multifaceted construct that is comprised of dissociable objective and subjective components (Fakhoury & Priebe, Reference Fakhoury and Priebe2002). The objective component pertains to observable features of individuals and their particular environments (e.g. employment, functional capacity, housing stability) and is apt to be more closely related to concepts of community functioning, whereas the subjective component captures satisfaction with one's experience in those environments (Ruggeri, Bisoffi, Fontecedro, & Warner, Reference Ruggeri, Bisoffi, Fontecedro and Warner2001). In the context of the broader psychiatric literature, our findings correspond to the pattern of associations between cognition and QoL reported in studies that parsed the objective and subjective dimensions. Indeed, whereas cognition consistently shows a modest, positive association with objective QoL, non-significant or inverse associations with subjective QoL have been reported in persons with schizophrenia (Tolman & Kurtz, Reference Tolman and Kurtz2012). The level of insight has been proposed as an explanation for the discrepancies between objective and subjective QoL ratings in schizophrenia patients (Hayhurst, Massie, Dunn, Lewis, & Drake, Reference Hayhurst, Massie, Dunn, Lewis and Drake2014) and could explain the lack of association between cognition and subjective QoL in the current study given the high rates of mental disorders in this sample (Tolman & Kurtz, Reference Tolman and Kurtz2012).
Previous work with this sample found resilience to confer a protective effect against poor mental health outcomes in the context of ACEs (Liu et al., Reference Liu, Mejia-Lancheros, Lachaud, Nisenbaum, Stergiopoulos and Hwang2020). We hypothesized that it would operate similarly in relation to functional outcomes and that it might further interact with cognition to buffer against poor outcomes. While resilience appeared to have a protective effect on QoL, we did not find any modification effects. In a study by Fazeli, Moore, and Vance (Reference Fazeli, Moore and Vance2019), resilience was identified as a mediator of the association between cognition and instrumental activities of daily living in persons with HIV, suggesting that erosion of cognitive capacity may diminish one's level of resilience and in turn negatively impact everyday functional abilities. Although it may be worthwhile to explore resilience from this perspective in future studies, our study did not show any substantial correlations between the initial level of cognitive functioning and resilience (see online Supplementary Table S2) suggesting that they may be operating independently in this sample.
One of the main limitations of this study is that the cognitive evaluation was brief and we were, therefore, unable to examine other dimensions of cognitive functioning, such as sustained attention, inhibitory control, and decision making, which are known to be impaired in homeless persons (Gicas et al., Reference Gicas, Vila-Rodriguez, Paquet, Barr, Procyshyn, Lang and Thornton2014). We also did not evaluate social cognition, yet it has been shown to account for more unique variance in functional outcomes (Halverson et al., Reference Halverson, Orleans-Pobee, Merritt, Sheeran, Fett and Penn2019; Horan et al., Reference Horan, Wynn, Gabrielian, Glynn, Hellemann, Kern and Green2019) and is positively correlated with resilience among homeless veterans (Greenberg et al., Reference Greenberg, Wynn, Lee, Hellemann, Gabrielian and Green2019). While our approach aimed to capture the dynamic relationship between cognition and outcomes via longitudinal modelling adjusting for common physical and mental health comorbidities, there are likely a number of other dynamic risk factors that were not measured, such as new incidents of traumatic brain injury or viral infection, states associated with heightened clinical symptomatology (e.g. acute depressive or manic episodes, active psychosis), or protective factors that may enhance functioning such as community integration. Nonetheless, the magnitude of positive associations between cognition and community functioning, and lack thereof for QoL, remained consistent over time. This suggests it is unlikely there was any substantial impact of unobserved time-dependent variables and instead suggests the impact of cognition on community functioning is likely to be reliable across time. Finally, it should be noted that homeless populations are inherently diverse and complex, and the heterogeneity of the demographic and clinical composition of any one sample will vary by geographic location making it difficult to generalize findings. The complexity of this population also makes it very difficult to recruit an adequate comparison group that has a similar demographic profile and life experience without the presence of psychiatric and physical illness comorbidities. However, this should not negate the value of examining the determinants of functioning within a local homeless community and the extent to which there are commonalities across communities. Given that cognition is a known predictor of functional outcomes across healthy and patient populations (Morgan & Heaton, Reference Morgan, Heaton, Grant and Adams2009), our findings within a homeless sample should be considered broadly relevant to the neuropsychological literature.
Overall, cognition is a clear contributor to community functioning in homeless adults. Current interventions for homeless persons offer recovery-oriented programs that mainly address needs in the area of housing, income, mental illness, and substance use (Aubry et al., Reference Aubry, Bloch, Brcic, Saad, Magwood, Abdalla and Pottie2020). Cognitive rehabilitation does not appear to be a core feature of existing models of care, but the findings from the current study support the view that building cognitive capacity could further optimize community functioning, which may, in turn, contribute to community integration and exiting homelessness. We could only locate two studies that have explicitly examined cognitive remediation programs in homeless adults (Medalia, Herlands, & Baginsky, Reference Medalia, Herlands and Baginsky2003) and youth (Medalia, Saperstein, Huang, Lee, & Ronan, Reference Medalia, Saperstein, Huang, Lee and Ronan2017), and although the sample sizes were small, there was evidence for cognitive gains that were greater than expected by chance or for practice effects. Cognitive rehabilitation should be considered a priority for homeless persons. Future research in this area should be oriented around how existing cognitive interventions could be adapted for this population, which would ideally involve randomized control trials to establish treatment efficacy. Importantly, intervention effectiveness studies will also need to be carried out and should be done so within integrated models of health and social care to optimize functioning and overall well-being outcomes. There is also a need to conduct future research that characterizes a broader scope of cognitive functions, such as social cognition and prospective memory, that may offer incremental predictive validity regarding functional outcomes and will better inform the development of cognitive interventions. More broadly, future research should aim to increase the representation of homeless females and youth (<25 years old) to better understand how their unique experiences and vulnerabilities may impact functioning and recovery (Luchenski et al., Reference Luchenski, Maguire, Aldridge, Hayward, Story, Perri and Hewett2018).
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291721001550.
Acknowledgements
The authors wish to thank the study participants for their time and willingness to share their life experiences to make the At Home/Chez Soi study possible. We are also grateful for the At Home/Chez Soi study team, coordinators, and service providers at the Toronto site who contributed to study development, implementation, and follow-up.
Financial support
This study was supported by financial contributions from the Mental Health Commission of Canada, the Canadian Institutes of Health Research (SWH, VS, CIHR MOP-130405), and the Ontario Ministry of Health and Long-term Care (SWH, VS, HSRF #259).
Conflict of interest
None.