



Overreliance on urine culture results in the absence of clinical signs and symptoms of infection has led to an epidemic of unnecessary antimicrobial use for asymptomatic bacteriuria (ASB). Reference Spivak, Burk and Zhang1,Reference Veillette, Waters and Gelman2 With the exception of select populations, guidelines recommend against antibiotics for ASB and treatment can lead to substantial harms, such as C. difficile infection, adverse drug events, and selective pressure, leading to antimicrobial resistance. Reference Nicolle3–Reference Köves, Cai and Veeratterapillay6 Diagnostic stewardship, with interventions targeted at culture ordering, processing, and reporting, is an emerging strategy to improve urinary tract infection (UTI) diagnosis. Reference Morgan, Malani and Diekema7,Reference Advani and Vaughn8
Studies of diagnostic stewardship interventions to limit the overdiagnosis and overtreatment of UTIs have targeted various stages of the diagnostic process. Reference Advani and Vaughn8–Reference Morado and Wong10 These interventions have led to significant decreases in unnecessary culturing and antimicrobials. These studies typically involve modifying only 1 step in the diagnostic process, and they describe research related to a quality improvement initiative, thus limiting generalizability. Importantly, most were performed without careful attention to implementation needs. Given these limitations, we conducted a modified-Delphi expert panel to identify best practices for urine-culture diagnostic stewardship. Reference Claeys, Trautner and Leekha11 Optimal implementation of these best practices, however, has not been described.
In this study, we assessed current practices and stakeholder perceptions of proposed urine-culture diagnostic stewardship interventions as part of a user-centered design process. We sought to refine intervention tools with end-user feedback to promote acceptance and sustained practice change as part of implementation in real-life settings.
Methods
Overall study design and sample
We used a qualitative descriptive design to better understand local practices and to assess perceptions of potential interventions related to the diagnostic pathway and diagnostic stewardship interventions for UTIs at participating Veterans’ Affairs Medical Centers (VAMCs). Reference Sandelowski12 Based on our previously published modified-Delphi expert guidance, interventions and associated tool prototypes were selected and developed within each of the 3 phases of urine-culture ordering, urine-culture processing, and urine-culture reporting. Reference Claeys, Trautner and Leekha11 The urine-culture ordering intervention consisted of informational nudges and required documentation of UTI signs and symptoms. An informational nudge is a tool used across many disciplines, originally in behavioral economics, to guide decision making while maintaining autonomy and often include framing the choice using positive and negative aspects of the decision. Reference Bearman, Morgan, Murthy and Hota13,Reference Thaler and Sunstein14 The urine-culture processing intervention focused on conditional urine culturing based on predefined urinalysis (UA) criteria of >10 urine white bloods cells per high-powered field (WBC/hpf). Reference Claeys, Trautner and Leekha11 The proposed urine-culture reporting interventions consisted of a nudge comment and selective antimicrobial reporting, such as cascade reporting.
We chose 3 geographically diverse VAMCs in which to implement this series of diagnostic stewardship interventions. These 3 sites did not have these interventions in place at the time of the study. A site-specific project lead who specialized in Infectious Diseases, Infection Prevention, and/or Antimicrobial Stewardship (AMS) was identified at each site prior to study initiation. In addition to serving as a key informant, each site-specific project lead helped to identify other potential interviewees directly or indirectly involved in the UTI diagnostic process. This purposeful sampling was used to access a focused group of key decision makers and stakeholders.
Recruitment
Using the list of names provided by each site-specific lead, we recruited a mix of stakeholders for interviews. These included frontline healthcare providers in various practice settings (ie, emergency department, acute care, home-based primary care, long-term care, and surgery), such as physicians and nurse practitioners, and those involved in urine-culture ordering, sample processing and/or antibiotic prescribing. All participants were employed at one of the selected study sites. Recruitment procedures included sending e-mails to solicit participation and up to 3 additional follow-up emails, as needed.
Intervention tool prototypes
Through work with the local Baltimore VA Medical Director of Informatics, we created prototype intervention tools for urine-culture ordering (Fig. 1) and reporting (Fig. 2) compatible with the VA Computerized Patient Record System (CPRS). We shared these low-fidelity visual display prototypes during each interview and encouraged end users to think aloud about using the tool in daily practice, including functionality from the user’s perspective, what type of prerequisite knowledge would be needed to use the tool, and whether there were design elements that would improve tool usability. Reference Reeder, Makic and Morrow15,Reference Richardson, Mishuris and O’Connell16 3 different prototypes for both ordering and reporting were available for comparison. For the processing phase, a prototype conditional urine-culturing workflow algorithm and criteria for a conditional reflex culture were also presented in visual form. The interviewees were asked for their opinion about the proposed process, terminology to describe the process, and the specified criteria.
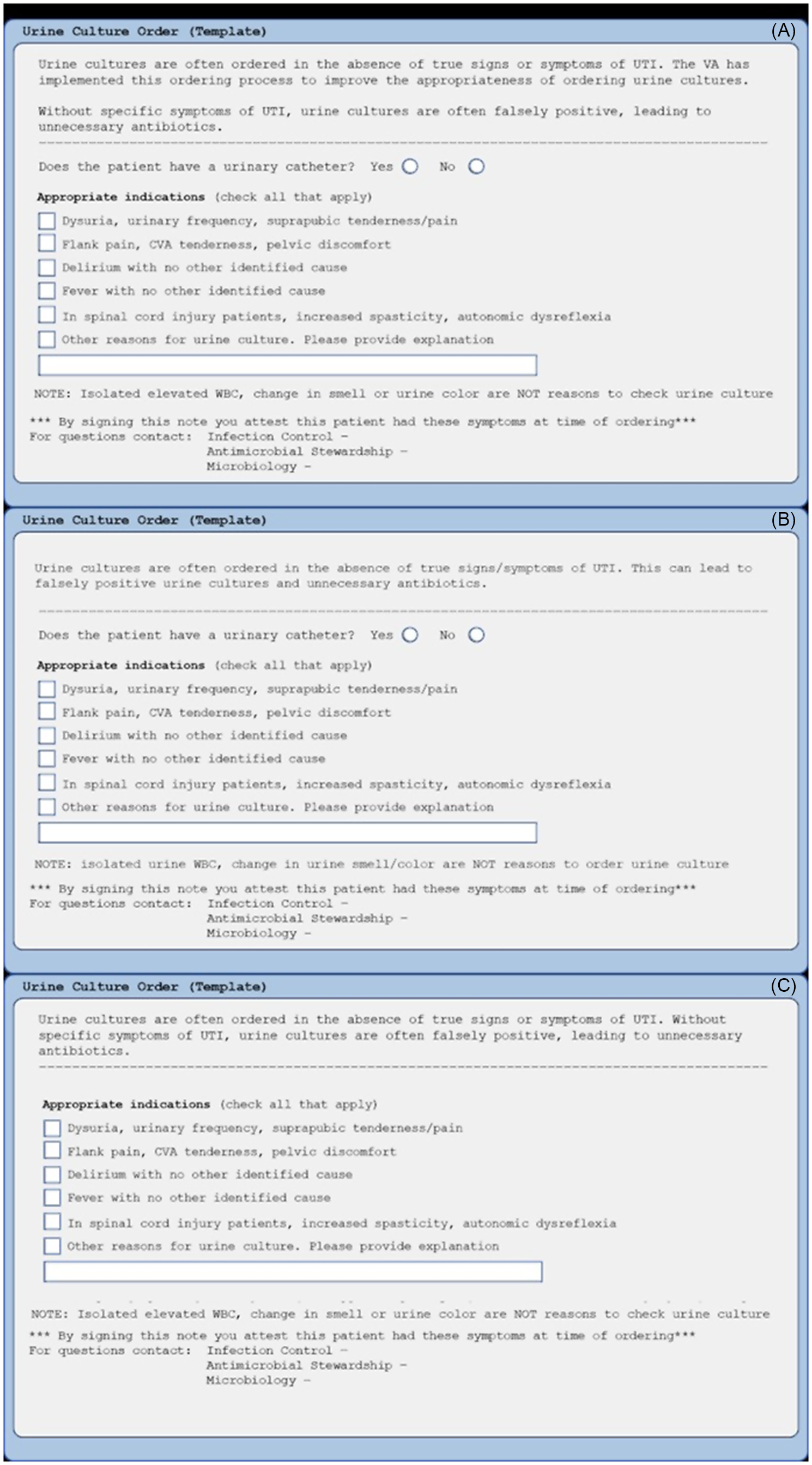
Figure 1. Low-fidelity prototype examples: urine-culture ordering tool. (A) Nudge advising against ordering urine cultures in the absence of signs and symptoms of infection, documentation of presence of urinary catheterization, order indications. (B) Nudge advising against ordering urine cultures in the absence of signs and symptoms of infection (less verbiage), documentation of presence of urinary catheterization, appropriate order indications. (C) Nudge advising against ordering urine cultures in the absence of signs and symptoms of infection, appropriate order indications.

Figure 2. Fidelity prototype examples: urine-culture reporting tool.
Data collection
The multidisciplinary research team, which included expertise in antimicrobial stewardship, infectious diseases, epidemiology, and qualitative research, developed a semistructured interview guide (Supplemental Appendix 1 online). The guide focused on determining current urine-culturing and treatment decision practices, as well as perceptions of the proposed interventions and prototype intervention tools for ordering, processing, and reporting of urine cultures. Concepts from the Consolidated Framework for Implementation (CFIR), primarily those related to the inner setting, intervention characteristics, and implementation process, informed the guide. Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery17 This structured interview guide allowed us to better understand current practices and inform prototype tool modifications and implementation strategies by identifying local barriers and facilitators, prior to implementation at each site. Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery17,Reference Safaeinili, Brown-Johnson, Shaw, Mahoney and Winget18 The interview guide was pilot tested with the 3 project leaders at each site, with minor adaptations based on their feedback.
Those who agreed to participate were scheduled for an individual interview with at least 2 study team members (S.L.K., L.W., and K.C.C.) with 1 team member leading the interview while the other took detailed notes. Interviews were completed virtually using VA-approved communication technologies (ie, Zoom.gov), given COVID-19 pandemic travel and site-visit limitations. Reference Archibald, Ambagtsheer, Casey and Lawless19 All interviews were audio recorded and transcribed using the VA Central Transcription Service to ensure accuracy and completeness, with the consent of the interviewee. The goal was to interview 10–15 individuals per study site. Participation was voluntary, and the interviewees did not receive study-related payments.
Data analysis
We used a rapid structured analysis or templated approach that focused on refining and implementing the intervention tools. Reference Averill20 Rapid analysis is an effective method for generating qualitative findings in a timely manner to facilitate further development and implementation of interventions in a fast-moving healthcare environment. Reference Gale, Wu and Erhardt21–Reference Lewinski, Crowley and Miller24 Specifically, we developed a summary template using key domains represented in the interview guide, which included the following: current practices with subdomains for culture ordering, processing, and result reporting; intervention tools with subdomains for potential usability and suggested improvements for each tool; and implementation with subdomains for barriers and facilitators. We used data from interview notes and transcripts to create a detailed summary for each individual interview according to these domains. Next, individual summaries were compiled and further summarized to create a detailed synthesis for each site incorporating perspectives from each interview participant, representing multiple professional roles. Finally, site summaries were used to construct a matrix to facilitate comparison across sites.
Results
Interviews were conducted between November 4, 2021, and May 23, 2022. Of the 77 healthcare personnel contacted, 31 consented to interview. The number of interviews ranged from 8 to 13 per site, and they were 29 to 63 minutes in length. The characteristics of the 3 hospitals are shown in Table 1 with a detailed description of interviewees available in Table 2.
Table 1. VA Medical Center Site Characteristics

Note. ICU, intensive care unit; SCI, spinal cord injuries and disorders; VA, Veterans’ Affairs; VA complexity level is determined through a model that includes information about patient population, clinical services, and teaching and research programs. Reference Fitzpatrick, Suda and Ramanathan41
a 2019 data, prior to COVID-19 pandemic.
Table 2. Interview Recruitment Characteristics, Overall and By Study Site

Note. AMS, antimicrobial stewardship; ID, infectious diseases; MD, medical doctor; NP, nurse practitioner; PA, physician assistant.
a Service chiefs were clinical care providers practicing in ambulatory care, emergency medicine, and hospital medicine.
b Other MD: CLC MD, home-base care MD, primary care MD, internal medicine MD.
c Other: medical lab supervisor, pathology and laboratory medicine service chief, health informatics officer, infection prevention BSN.
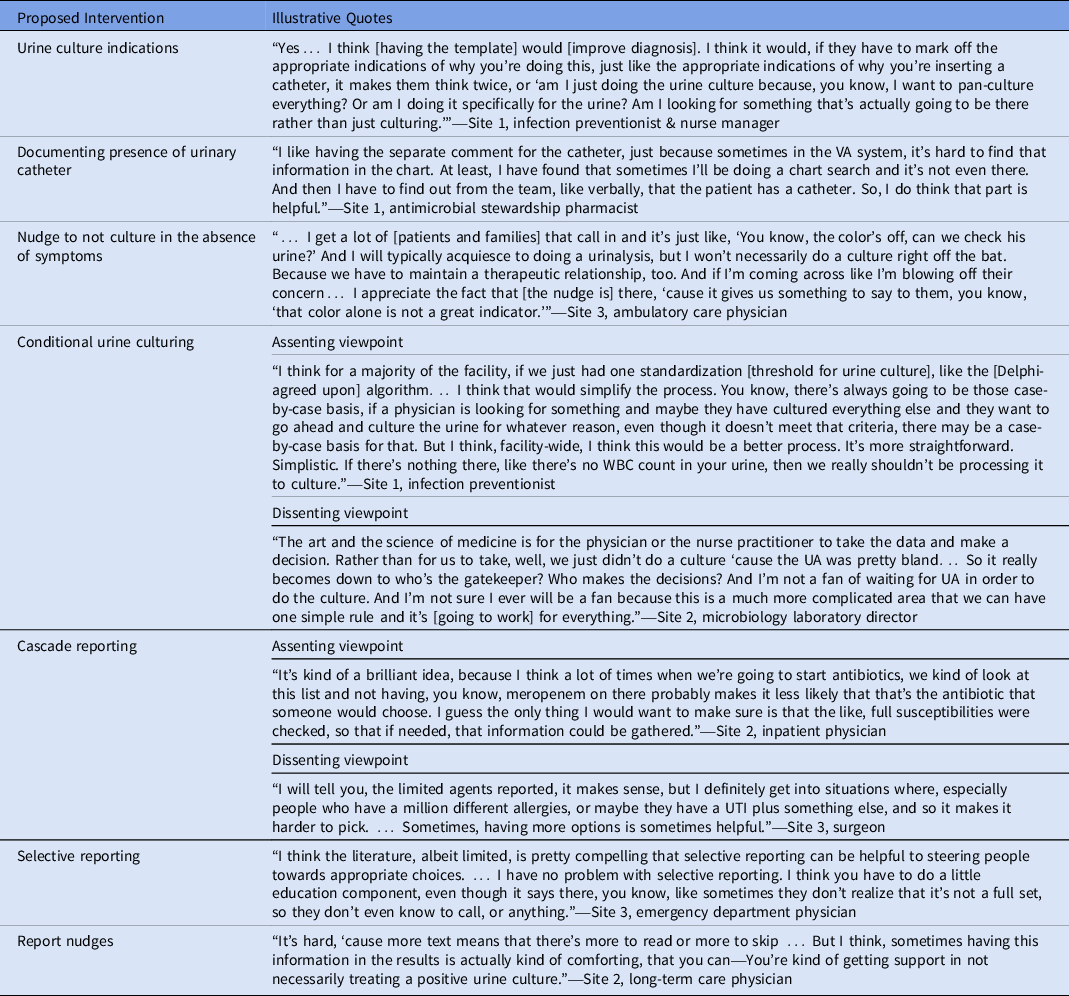
Table 3. Illustrative Participant Quotes by Intervention Component
All 3 sites, though geographically diverse, consisted of at least 1 acute-care hospital with 1 or more long-term care units, and ambulatory outpatient clinics. Average census varied, but all sites were classified as high-complexity facilities and had level 1 intensive care units. Also, 2 sites had spinal cord injury centers and 2 sites had immunocompromised patients treated within transplant centers. None of the sites had a dedicated diagnostic stewardship group. Aligned with joint commission requirements, all 3 sites had a physician-led AMS program, though the activities related to UTI diagnosis and treatment interventions varied substantially across the sites.
Our main findings within each domain of urine-culture ordering, processing, and reporting of urine cultures are discussed in further detail below, with an emphasis on notable differences and common challenges across sites, as well as preferences and suggestions related to the interventions and prototype intervention tools. Illustrative quotes for proposed interventions across each domain are presented in Table 3.
Urine-culture ordering
Across all 3 sites, urine-culture ordering was primarily physician driven, but nurse-driven protocols also influenced how and when urine cultures were ordered. Sites 1 and 2 did not have aids for assisting in urine-culture ordering, whereas site 3 had clinical decision support (CDS) to assist providers in differentiating whether patients potentially had ASB versus true infection. Decisions surrounding appropriate indications for when to order urine cultures were consistent across the 3 sites, except sites 1 and 2 had annual screening cultures for spinal cord injury patients.
Overall, interviewees at all sites agreed that requiring the identification and documentation of UTI related clinical signs and symptoms would improve culture ordering practices and UTI diagnosis, and they were supportive of the proposed intervention. The preferred CPRS-integrated urine-culture ordering template had less verbiage for the informational nudge. As few “clicks” as possible were deemed essential to successful integration of this tool. Most participants at all 3 sites supported documentation of catheterization for frontline-provider awareness and decision making at the point of care, as well as data collection for quality improvement projects because catherization can be a dynamic process that is not always accurately documented in the electronic medical record (EMR).
Urine-culture processing
Processing of urine cultures and perceptions of the proposed intervention of conditional urine reflex culturing varied across the 3 sites. Although participants at site 1 were eager to implement conditional urine reflex testing, a key stakeholder at site 2 did not want any form of conditional linkage of UA and urine culture implemented because they did not believe it would be an effective use of resources. Additionally, site 3 had previously implemented a different restrictive culture practice in collaboration with urology. At site 3, urine cultures were conditionally cancelled if they met the following criteria: UA nitrite was negative, ≤5 WBC/hpf, and microscopy was negative for both bacteria and yeast. All 3 sites, however, had similar processes for how UAs and urine cultures were initially processed. Moreover, many respondents at all 3 sites agreed upon the utility of conditional urine reflex testing and the Delphi agreed upon-urine WBC threshold of >10 WBC/hpf to proceed with urine culturing.
Urine-culture reporting
All 3 sites had similar mechanisms to report culture results. Site 2 had already implemented some form of selective reporting by restricting fluoroquinolone susceptibility information. For sites 1 and 2, all aspects of urine-culture reporting were completed on site. Site 2 had 3 acute-care hospitals; the processing was centralized to 1 clinical microbiology laboratory. For site 3, after initial processing, urine cultures were sent to a nearby affiliated VAMC for automated antimicrobial susceptibility testing. Notably, this limited the autonomy of site 3 with respect to interventions related to urine-culture reporting, but interviewees agreed that collaboration with the external site was possible.
When presented with different CPRS-compatible urine-culture report prototypes, there was considerable support for either use of cascade reporting or a report that highlights national and/or local guideline recommended agents. Cascade reporting would first report IDSA-recommended narrow-spectrum agents, with secondary more broad-spectrum agents reported based on resistance patterns. Many liked the idea of cascade reporting but were unsure of the feasibility of implementing this approach. Stakeholders working in clinical microbiology laboratories strongly disagreed with inclusion of a statement to call the laboratory to request further susceptibilities, stating that this would negatively impact workflow. If cascade reporting was deemed infeasible, a report that included a note regarding the preferred antimicrobial agents while maintaining a comprehensive list of antimicrobial susceptibilities was considered desirable.
Implementation considerations
All 3 sites stressed the importance of providing clinicians with education about changes occurring at their respective health systems, including the clinical reasoning behind the changes and what to expect in terms of timeline and impact on daily workflow. Involvement of AMS programs and local champions was identified as essential for implementation success. One interviewee commented:
“… Obviously, you’ve got the [antimicrobial] stewardship folks, whoever is engaged in stewardship, and then you really need—what’s often lacking is the ED champion… you really need someone who speaks the lingo to give the perspective of that frontline provider… show the value of why this is going to help them.” (Site 3 emergency department MD)
Overall, participants at site 1 were eager to begin implementing all changes and suggested collaboration with AMS to ensure that education on the changes made it through all relevant providers. Participants at site 2 were more hesitant about the proposed interventions, especially those affecting the clinical microbiology laboratory. Interviewees noted that buy-in from service and section chiefs would be needed to ensure successful implementation. Participants at site 3 were amenable to the proposed changes, but they were also concerned about some potential barriers to implementation. Their first concern was the transition from CPRS to CERNER software, and their second concern was the existing local collaborations with other medical centers for specific services.
Discussion
Through interviews with providers and other personnel involved in the UTI diagnostic process, we not only learned about existing policies and procedures for diagnosis and management of UTIs but also gained important insights about implementing diagnostic stewardship interventions at each VAMC. Across and within sites, we detected differences in diagnostic and management practices for UTIs. Some sites had multiple campuses and others had off-site clinical microbiology. The results of these interviews highlight the importance of understanding local barriers and facilitators, which can help tailor interventions and educational activities to enable adoption and long-term integration. Using a practical implementation checklist (Fig. 3) and low-fidelity visual display prototypes, we were able to gain insight into how to alter our proposed interventions to better align with current practices and available resources at each site.

Figure 3. Checklist of key considerations for diagnostic stewardship implementation.
Several interventions have been proposed at the phase of ordering urine cultures to decrease unnecessary testing. Improved provider education, diagnostic algorithms, and indication-based order sets have been shown to improve UTI diagnostic accuracy. Reference Egger, Balmer, Friedli-Wüthrich and Mühlemann25–Reference Watson, Trautner and Russo29 These interventions tend to be labor intensive. Consequently, many have chosen to leverage the EMR to aid in decreasing urine culturing. Reference Shirley, Scholtz, Osterby, Musuuza, Fox and Safdar30–Reference Lin, Knowlson and Nguyen32 An expert panel recommended requiring documentation of signs and symptoms of UTI as an important cognitive double check before ordering urine cultures. Across all sites, interviewees agreed that documentation would be beneficial; however, some were concerned about interrupting workflow and emphasized the need for the ordering process to be clear and concise, with the least amount of verbiage and clicks as possible. The ordering prototype was adjusted to reflect this feedback, and a note was made to ensure that local implementation would not lead to multiple additional steps in the ordering process within the EMR.
The UA and urine culture are typically processed separately. Results from the UA, however, can be used to guide decision making for urine culturing. Numerous studies have demonstrated that limiting urine culturing based on UA results can assist in decreasing unnecessary work-up of urinary specimens. Reference Claeys, Zhan and Pineles33–Reference Howard-Anderson, Ashraf, Overton, Reif, Murphy and Jacob37 By conditionally cancelling urine cultures if specific criteria are not met on UA, clinical microbiology laboratories can decrease test volume. Of the 3 sites, representatives at 2 sites were supportive of this process, and 1 site had implemented a modified version of this practice. One site had a key stakeholder who was adamantly opposed. The proposed protocol was adjusted to address specific site concerns for feasibility, while also incorporating the modified-Delphi recommended urine WBC cutoff of >10 WBC/hpf. Reference Claeys, Trautner and Leekha11 Through the interviews, we also identified the stakeholders’ need for protocol implementation within the clinical microbiology laboratories and laboratories responsible for UA processing, and we developed specific education to address concerns about laboratory workflow.
Urine-culture reporting tended to be the most diverse and divisive issue among all 3 sites. Forms of cascade reporting have been proposed by the Clinical Laboratory Standards Institute and studied at VA and non-VA medical centers. Reference Vissichelli, Orndahl and Cecil38–40 Those who supported cascade reported were unsure of local feasibility. Those against cascade reporting did not like how provider autonomy would be limited and worried that it would lead to more calls to the microbiology laboratory that would interrupt workflow. Most interviewees were supportive of providing informational nudges to decrease unnecessary testing and direct providers to guideline-based therapy recommendations. This led to the decision to pursue informational nudges first to facilitate implementation, followed by discussion on selective restriction of reporting (ie, restricting fluoroquinolones) and to forgo further discussion of cascade reporting. Feedback from each site is also being used to develop individual reporting plans and educational initiatives in collaboration with local AMS programs.
Our study had several limitations. The interviews were conducted at 3 purposely selected VAMCs as part of research; the sample, though geographically diverse, cannot be generalized to all VAMCs or healthcare systems outside the VA. There is also a risk of response bias among those interviewed. To minimize this bias, we interviewed individuals from diverse professional backgrounds and organizational roles, obtaining both clinical and nonclinical perspectives at each respective facility. This analysis is also largely descriptive and does not provide an in-depth examination of underlying factors that contribute to the organizational culture of UTI diagnosis and management at each participating facility. Interpretation bias was also possible based on the study teams’ perspectives and professional experiences. This bias was mitigated by ensuring a diverse interdisciplinary study team, which met regularly to discuss and interpret data collection and results analysis.
The overdiagnosis of UTI and inappropriate treatment of ASB has been well established in the medical literature. Additionally, systematic application of diagnostic stewardship interventions has been shown to limit culturing and, thereby, reduce unnecessary use of antibiotics at a minimal cost and without adverse consequences. Widespread implementation of these diagnostic stewardship interventions, however, has been limited. This study, through the positive response and support of those interviewed, both informs and highlights opportunities for implementation of 3 novel urine-culture diagnostic stewardship interventions.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ice.2023.106
Acknowledgments
The contents do not represent the views of the US Department of Veterans’ Affairs or the US government.
Financial support
This work was supported by the US Department of Veterans’ Affairs Health Services Research and Development Service (Merit Award No. 1I01HX002906-01A1 and RSC 5IK6HX003399-03), and National Academy of Medicine Scholars in Diagnostic Excellence Program.
Competing interests
K.C.C. reports speaking and advisory roles with bioMérieux. All other authors report no relevant conflicts of interest.








